What is the MPFS (Medicare Physician Fee Schedule) in Healthcare?
The Medicare Physician Fee Schedule (MPFS) is the official payment system used by Medicare to determine how physicians and other qualified healthcare professionals are reimbursed for covered services. Established under the Resource-Based Relative Value Scale (RBRVS) in 1992, the MPFS standardizes payment rates nationwide while allowing adjustments for regional cost variations through the Geographic Practice Cost Index (GPCI).
Under the MPFS, every CPT or HCPCS Level II code is assigned a Relative Value Unit (RVU) representing the relative cost of performing that service. RVUs are divided into three components:
- Physician Work RVU — The time, skill, and effort required.
- Practice Expense RVU — The overhead and supplies necessary to perform the service.
- Malpractice RVU — The cost of professional liability insurance.
Each component is adjusted by the appropriate GPCI value to account for local cost differences. The total is then multiplied by the annual Medicare Conversion Factor (CF) — a dollar value set by CMS — to calculate the final reimbursement amount.
Formula:
Payment = [(Work RVU × Work GPCI) + (PE RVU × PE GPCI) + (MP RVU × MP GPCI)] × Conversion Factor
The MPFS applies to Medicare Part B services, including outpatient visits, procedures, diagnostic testing, and telehealth. It is the foundation for both public and private payer reimbursement models, as many commercial insurers benchmark their payments to MPFS rates.
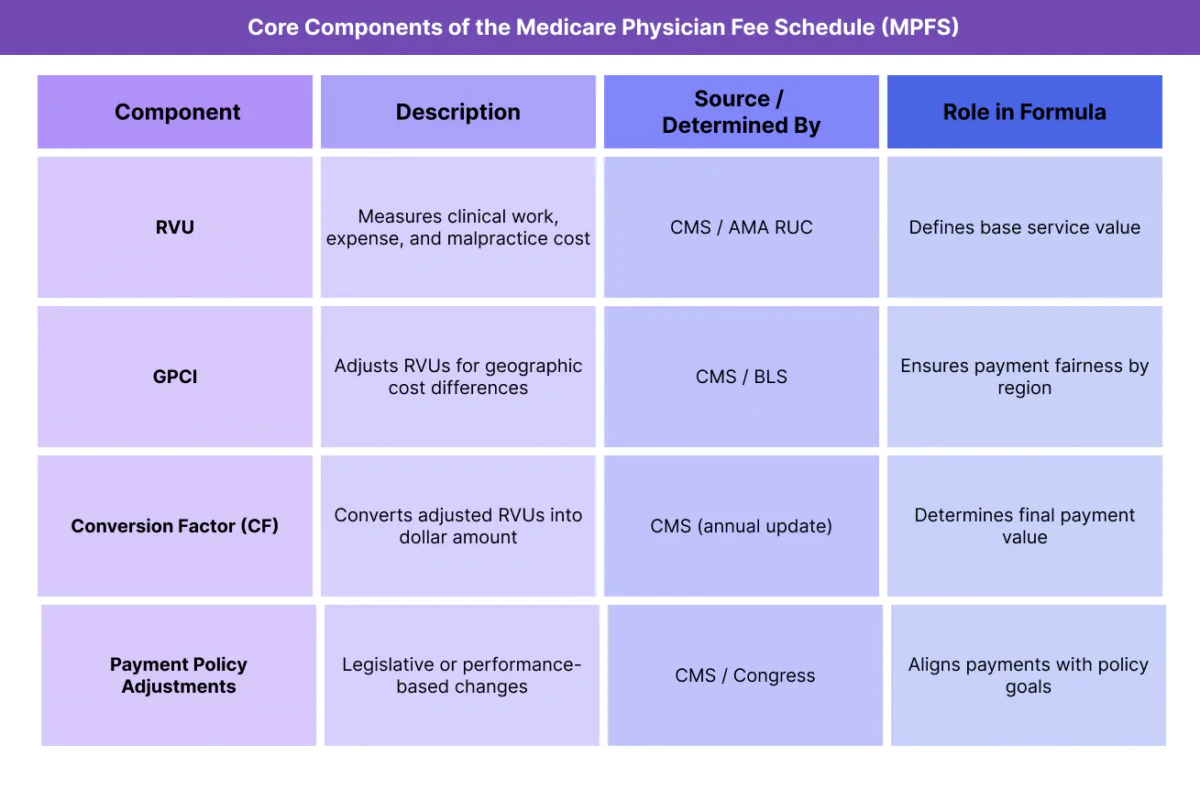
Key Components of the Medicare Physician Fee Schedule (MPFS)
The Medicare Physician Fee Schedule (MPFS) determines the amount Medicare pays physicians and other qualified health professionals for covered services. It combines clinical valuation, geographic adjustment, and federal policy updates into a standardized national framework.
The MPFS payment rate for each CPT® or HCPCS code is determined by multiplying the Relative Value Units (RVUs) by the Geographic Practice Cost Index (GPCI) and then by the Conversion Factor (CF) — the dollar amount assigned by CMS each calendar year.
1. Relative Value Units (RVUs)
Represent the relative cost and resource intensity of each service.
Divided into three categories:
- Work RVU — Time, effort, and skill required by the physician.
- Practice Expense (PE) RVU — Cost of staff, supplies, and overhead.
- Malpractice (MP) RVU — Cost of professional liability insurance.
Developed and maintained by CMS in collaboration with the American Medical Association (AMA) through the Relative Value Scale Update Committee (RUC).
2. Geographic Practice Cost Index (GPCI)
- Adjusts each RVU component to reflect regional cost-of-living differences.
- Calculated separately for work, practice expense, and malpractice.
- Ensures equitable payment for providers across high- and low-cost regions.
3. Conversion Factor (CF)
- Converts the total adjusted RVUs into a dollar payment amount.
- Updated annually by CMS and published in the Federal Register.
- Influenced by factors such as the Medicare Economic Index (MEI), federal budget neutrality rules, and Congressional mandates.
4. Payment Policy Adjustments
- CMS applies additional modifiers and adjustments to reflect legislative and policy requirements, including:
- Budget neutrality adjustments.
- Statutory payment limits or sequestration.
- Quality Payment Program (QPP) incentives or penalties under MIPS/APMs.
These modifications ensure Medicare spending remains balanced while rewarding performance and value.
5. Annual Update Process
- CMS updates the MPFS each year through a proposed rule (mid-year) and final rule (late-year) process.
- Stakeholders — including specialty societies, professional organizations, and policymakers — provide input during public comment periods.
- The finalized payment rates take effect on January 1 of the following year.
How the Medicare Physician Fee Schedule (MPFS) Works in Practice
The Medicare Physician Fee Schedule (MPFS) governs how physicians and qualified healthcare professionals are paid for covered services under Medicare Part B. It is applied automatically by CMS and Medicare Administrative Contractors (MACs) during claims processing to calculate allowed amounts and provider reimbursement.
The MPFS workflow links the clinical documentation and coding process to the financial outcome, ensuring consistency across providers, regions, and service types.
Step 1: Service Documentation and Code Selection
- Providers document patient encounters in the electronic health record (EHR) according to medical necessity and service performed.
- The documentation is translated into the appropriate CPT or HCPCS Level II codes, which define the service or procedure billed to Medicare.
- Each code is assigned specific RVUs under the Resource-Based Relative Value Scale (RBRVS).
Step 2: Apply Geographic Adjustments (GPCI)
- CMS uses the provider’s practice ZIP code to determine the applicable GPCI values (for Work, Practice Expense, and Malpractice).
- The corresponding RVUs are multiplied by those GPCI factors to create geographically adjusted RVUs.
Step 3: Convert to a Dollar Amount
- The total adjusted RVUs are multiplied by the Medicare Conversion Factor (CF) — a dollar amount updated annually by CMS.
- This step translates the relative value into the final Medicare-allowed amount.
- Formula:
Payment = [(Work RVU × Work GPCI) + (PE RVU × PE GPCI) + (MP RVU × MP GPCI)] × Conversion Factor
Step 4: Claim Submission and Payment Processing
- The claim is submitted electronically via CMS-1500 or 837P format to the Medicare Administrative Contractor (MAC).
- The MAC applies the MPFS to verify the payment rate, check modifier use, and confirm provider eligibility.
- Payment is issued directly to the provider (or group) as the Medicare allowable reimbursement, less patient cost-sharing (coinsurance or deductible).
Step 5: Integration with Quality and Performance Programs
- The MPFS interacts directly with CMS quality programs like the Merit-Based Incentive Payment System (MIPS) and Advanced Alternative Payment Models (APMs).
- Providers may receive positive or negative payment adjustments based on performance scores, which modify the standard MPFS reimbursement rate.
- Many commercial payers benchmark their reimbursement contracts on MPFS rates, applying proprietary multipliers (e.g., 110% of MPFS).
MPFS Billing, Reimbursement, and Program Limitations
The Medicare Physician Fee Schedule (MPFS) defines how Medicare reimburses for Part B professional services and procedures. It is the most widely used payment framework in U.S. healthcare — not only for Medicare but also as a benchmark for commercial payers, Medicaid programs, and value-based care contracts.
While it provides transparency and consistency, the MPFS is also constrained by budget neutrality laws, conversion factor adjustments, and administrative complexity, all of which influence provider compensation year over year.
How MPFS Determines Reimbursement
- Each CPT or HCPCS code’s payment is calculated by multiplying RVUs (work, practice expense, malpractice) by GPCI adjustments and then by the Conversion Factor (CF).
- The Conversion Factor converts the adjusted RVUs into a dollar value and is updated annually by CMS.
- Payment rates are published each year in the Medicare Physician Fee Schedule Final Rule, effective January 1.
- Most other payers (including commercial carriers) base their contracts on MPFS benchmarks, typically paying a percentage above or below Medicare’s rates.
Budget Neutrality and Conversion Factor Adjustments
- CMS must maintain budget neutrality, meaning any increases in RVUs or policy changes that raise total spending must be offset by reductions elsewhere — usually in the Conversion Factor.
- This mechanism often leads to small annual payment cuts, even when code values or volumes increase.
- The Conversion Factor has declined steadily in recent years, from $36.09 in 2020 to around $32 in 2025, largely due to congressional budget constraints.
- CMS may apply temporary relief measures, such as statutory freezes or inflation adjustments, to stabilize payment levels.
Common Billing and Reimbursement Challenges
- Documentation Demands: Accurate coding and supporting documentation are critical to avoid denials or compliance risks.
- Modifier Use: Improper or missing modifiers (e.g., -25, -59, -95) can delay payment or trigger audits.
- Telehealth Expansion: While many telehealth services were added to the MPFS during the COVID-19 Public Health Emergency, reimbursement parity remains inconsistent across codes and payers.
- Complexity Across Payers: Because many private insurers apply different GPCI mappings or proprietary conversion factors, the same service may reimburse differently depending on payer.
Limitations and Policy Concerns
- Annual Instability: Year-to-year adjustments in the Conversion Factor create financial uncertainty for providers.
- Underpayment for Cognitive Services: Critics argue that procedural specialties are overvalued relative to primary care under the RVU weighting system.
- Geographic Inequity: Even with GPCI adjustments, the MPFS may not fully reflect the true cost of care in rural or high-cost areas.
- Legislative Dependence: Major MPFS reforms often require congressional action, slowing responsiveness to economic changes.
MPFS and Its Impact on Quality, Access, and Health Equity
The Medicare Physician Fee Schedule (MPFS) not only defines how clinicians are reimbursed but also shapes the incentives that drive care quality, access, and equity across the U.S. healthcare system. Because most commercial and state payers benchmark their rates against the MPFS, its structure affects nearly every aspect of physician practice economics — from service volume and specialty mix to rural workforce distribution.
Advancing Payment Transparency and Standardization
- MPFS provides a nationally uniform payment framework, ensuring predictable reimbursement for the same service regardless of payer.
- The structure simplifies contract negotiations and reduces arbitrary variation in pricing, creating a transparent baseline for both providers and payers.
- This consistency improves accountability and facilitates data-driven payment policy development by CMS.
Encouraging Quality and Value-Based Care
- The MPFS underpins programs like the Quality Payment Program (QPP) and Merit-Based Incentive Payment System (MIPS), which link reimbursement to performance metrics.
- Providers demonstrating quality outcomes or engaging in Advanced Alternative Payment Models (APMs) can receive upward adjustments, aligning clinical excellence with financial reward.
- However, the traditional fee-for-service (FFS) foundation of MPFS still tends to reward volume over value, creating tension with modern care coordination models.
Impact on Access and Provider Distribution
- Because GPCI adjustments and conversion factors can fluctuate, payment disparities persist between urban and rural regions.
- Primary care and cognitive specialties often face lower reimbursement relative to procedural fields, making it harder to attract and retain clinicians in underserved areas.
- CMS has introduced targeted incentives and programs — such as HPSA bonuses, telehealth coverage, and rural add-on payments — to partially offset these gaps.
Promoting Health Equity Through Payment Policy
- The MPFS serves as a key lever for health equity reform, with CMS using its annual rulemaking process to promote access and reduce systemic disparities.
- Policy changes often prioritize coverage expansion for preventive, behavioral health, and chronic care management services, which improve outcomes for historically underserved populations.
- Still, some equity goals are constrained by budget neutrality, limiting CMS’s ability to make large-scale redistributive adjustments without congressional action.
Long-Term Outlook for Fairness and Sustainability
- The future of MPFS lies in hybrid payment models that blend traditional FFS with value-based and population health incentives.
- Policymakers continue to explore reforms to rebalance reimbursement between specialties and strengthen rural access.
- Modernizing MPFS to better reflect clinical complexity, care coordination, and equity goals will be essential to maintaining quality and sustainability in Medicare’s physician payment system.
Frequently Asked Questions about the MPFS
1. What is the Medicare Physician Fee Schedule (MPFS)?
The Medicare Physician Fee Schedule (MPFS) is the payment system used by CMS (Centers for Medicare & Medicaid Services) to reimburse physicians and qualified healthcare professionals for services covered under Medicare Part B. It assigns standardized payment rates to CPT® and HCPCS codes using the RBRVS formula, adjusted for geography through GPCI and converted into a dollar amount using the Conversion Factor (CF).
2. How are MPFS payment rates calculated?
Each code’s payment is calculated using this formula:
Payment = [(Work RVU × Work GPCI) + (Practice Expense RVU × PE GPCI) + (Malpractice RVU × MP GPCI)] × Conversion Factor
This formula combines the service’s relative value (RVUs), geographic cost differences (GPCI), and the national dollar multiplier (CF) to produce the final Medicare-allowed amount.
3. What is the difference between MPFS and RBRVS?
- RBRVS (Resource-Based Relative Value Scale): The underlying valuation system that assigns RVUs to medical services.
- MPFS: The complete reimbursement schedule that applies GPCI adjustments and the Conversion Factor to those RVUs to determine payment.
In short, RBRVS defines value; MPFS defines payment.
4. How does MPFS differ from the All-Inclusive Rate (AIR)?
- MPFS: Applies to individual services billed under Medicare Part B, paying per CPT® or HCPCS code.
- AIR (All-Inclusive Rate): Used by Rural Health Clinics (RHCs), reimbursing one encounter-based payment per qualifying visit under a cost-based model.
Both systems promote equitable reimbursement, but AIR focuses on clinic-level costs while MPFS focuses on service-level values.
5. Who updates the MPFS and how often?
CMS updates the MPFS annually through the Federal Register rulemaking process, which includes a proposed rule (typically midyear) and a final rule (issued late in the year). Updates take effect January 1 each year and reflect new CPT® codes, RVU changes, and policy adjustments.
6. What is the Medicare Conversion Factor (CF)?
The Conversion Factor is the dollar multiplier used to convert total adjusted RVUs into a payment amount. It changes each year based on inflation (MEI), budget neutrality requirements, and congressional mandates. Even small CF adjustments can significantly affect overall physician reimbursement.
7. Why is the MPFS important beyond Medicare?
The MPFS sets the national benchmark for physician reimbursement across the healthcare industry. Many private insurers and Medicaid programs base their own fee schedules on MPFS rates, often applying a percentage multiplier (e.g., 110% of MPFS). As a result, MPFS changes influence nearly all payer contracts and healthcare economics nationwide.
