What is the GPCI (Geographic Practice Cost Index) in Healthcare?
The Geographic Practice Cost Index (GPCI) is a Medicare adjustment factor used to modify physician reimbursement rates based on regional cost differences. Established under the Resource-Based Relative Value Scale (RBRVS) system, the GPCI ensures that payments under the Medicare Physician Fee Schedule (MPFS) reflect the local cost of delivering care — including variations in wages, rent, malpractice premiums, and practice expenses.
Each CPT or HCPCS code under the MPFS has three core components: physician work, practice expense, and malpractice expense. The GPCI assigns a regional multiplier to each of these elements to adjust the code’s Relative Value Units (RVUs) for local economic conditions.
In practical terms, the GPCI ensures that a physician in a high-cost area like San Francisco receives a higher payment for the same service than a provider in a lower-cost region. This approach maintains payment equity across the U.S. while preventing excessive regional disparities.
The GPCI is updated periodically by the Centers for Medicare & Medicaid Services (CMS) using data from the Bureau of Labor Statistics (BLS) and other federal sources. It is applied in the formula that determines Medicare payment:
Payment = [(Work RVU × Work GPCI) + (Practice Expense RVU × PE GPCI) + (Malpractice RVU × MP GPCI)] × Conversion Factor
Key Components of the Geographic Practice Cost Index (GPCI)
The Geographic Practice Cost Index (GPCI) adjusts Medicare reimbursement to reflect regional variations in the cost of providing care. Each Relative Value Unit (RVU) in the Resource-Based Relative Value Scale (RBRVS) is multiplied by a corresponding GPCI value based on the provider’s practice location.
GPCI values are calculated for each Medicare locality across the United States and vary annually based on updated federal cost data.
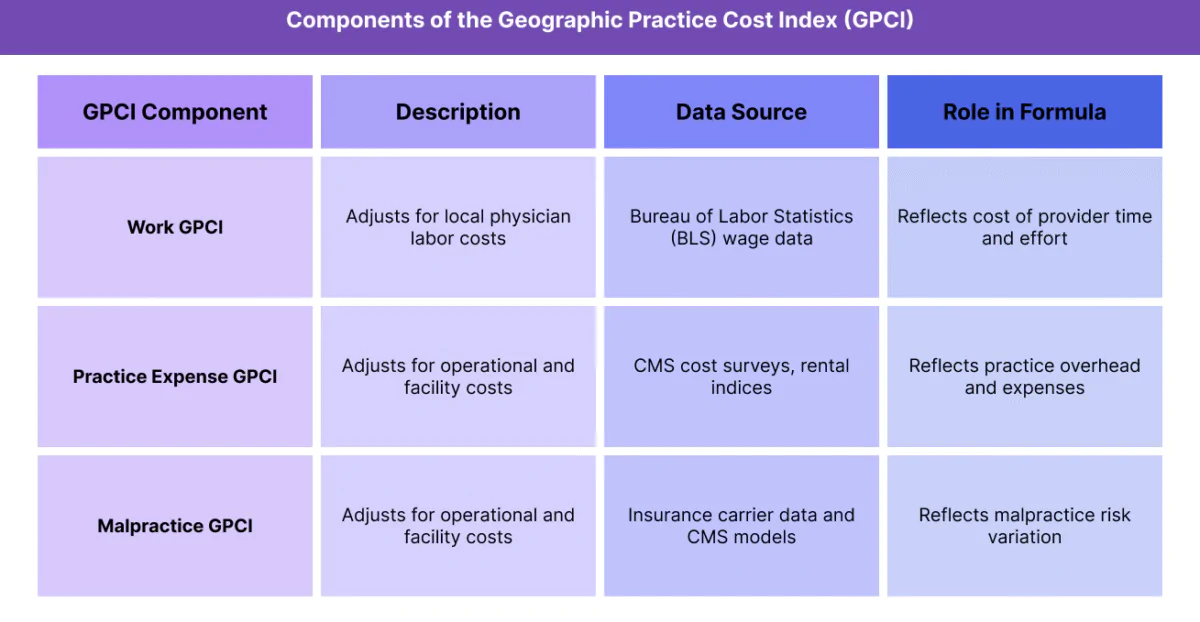
1. Work GPCI (Physician Labor Component)
- Reflects the cost of physician labor and professional time required to perform a service in a given region.
- Influenced primarily by local wage levels and labor market data from the Bureau of Labor Statistics (BLS).
- Accounts for roughly 50% of the total RVU adjustment in most specialties.
- Ensures that physician compensation reflects regional cost-of-living differences.
2. Practice Expense (PE) GPCI
- Represents the overhead and operational costs of running a medical practice.
- Includes expenses such as staff wages, office rent, utilities, equipment, and medical supplies.
- Varies significantly by location, since facility and labor costs differ widely between rural and urban settings.
- Often the largest driver of variation in regional reimbursement.
3. Malpractice (MP) GPCI
- Adjusts for geographic differences in professional liability insurance premiums.
- Derived from insurance rate data compiled by CMS and industry sources.
- Typically the smallest component, but critical for maintaining fairness in high-risk states where malpractice costs are substantial.
How the Three GPCIs Work Together
Each CPT code’s total RVUs are multiplied by their respective GPCI values, producing a geographically adjusted total RVU.
That value is then multiplied by the Medicare Conversion Factor to calculate the final reimbursement amount.
This structure allows CMS to standardize relative value assignment nationally while still accounting for local economic realities that affect practice costs.
How the GPCI (Geographic Practice Cost Index) Works in Practice
The Geographic Practice Cost Index (GPCI) is applied automatically within the Medicare Physician Fee Schedule (MPFS) during claim adjudication to ensure regional payment accuracy. It is one of the three adjustment factors—alongside RVUs and the Conversion Factor—that determine the final Medicare payment rate for a given CPT or HCPCS code.
GPCI values are assigned to every Medicare payment locality, and all Part B claims are adjusted according to the provider’s practice ZIP code.
Step 1: Identify the Service and Base RVUs
- Each CPT or HCPCS code under the Resource-Based Relative Value Scale (RBRVS) includes three RVU components: Work, Practice Expense, and Malpractice.
- These unadjusted RVUs represent the national relative resource cost for providing the service.
Step 2: Apply the GPCI Adjustments
CMS multiplies each of the three RVU components by the corresponding GPCI values for the provider’s geographic area:
- Work RVU × Work GPCI
- Practice Expense RVU × PE GPCI
- Malpractice RVU × MP GPCI
The resulting geographically adjusted RVUs reflect local cost variations.
Step 3: Combine and Multiply by the Conversion Factor
The sum of the adjusted RVUs is then multiplied by the Medicare Conversion Factor (CF), which converts the total relative value into a dollar payment amount.
Formula:
Payment = [(Work RVU × Work GPCI) + (PE RVU × PE GPCI) + (MP RVU × MP GPCI)] × Conversion Factor
The resulting value is the final Medicare-allowed amount for that service in the provider’s locality.
Step 4: Use in Claims Processing and Reporting
- Billing systems automatically apply GPCI values when calculating expected Medicare payments.
- Providers can review their local GPCI values in CMS’s annual MPFS update files, published in the Federal Register and CMS’s public data sets.
- GPCI adjustments also influence Medicaid and commercial payer contracts, as many private insurers benchmark their reimbursement models on Medicare rates.
Step 5: Ongoing Updates and Policy Oversight
- CMS reviews and updates GPCI data every three years based on new cost indices, with interim adjustments as needed for accuracy.
- Regional disparities in cost-of-living, rent, and malpractice premiums are continually monitored to maintain payment equity across the nation.
GPCI Billing, Reimbursement, and Program Limitations
The Geographic Practice Cost Index (GPCI) is a vital part of Medicare’s payment equity framework, ensuring that providers are reimbursed according to the regional cost of delivering care. However, while it brings fairness to national payment structures, it also introduces complexities, disparities, and political challenges in balancing local variation and federal standardization.
How GPCI Affects Reimbursement
- Each CPT or HCPCS code’s reimbursement under the Medicare Physician Fee Schedule (MPFS) is adjusted using GPCI values tied to the provider’s practice location.
- Higher-cost regions (urban areas with elevated wages and rents) receive higher adjusted payments, while lower-cost rural areas receive less.
- This ensures economic consistency in compensation but can unintentionally widen urban–rural payment gaps when operational costs don’t align with the formula’s assumptions.
- GPCI adjustments apply only to the non-facility component of care; facility payments (hospital outpatient, RHC, FQHC) are determined by separate CMS methodologies.
Payment Calculation Impact
The three GPCI components—Work, Practice Expense, and Malpractice—each influence reimbursement differently:
- Work GPCI: Reflects wage differentials; highest influence on total payment.
- Practice Expense GPCI: Reflects office cost and rent differences; varies most across regions.
- Malpractice GPCI: Smallest impact but important for high-risk specialties.
CMS caps the overall payment adjustment range to maintain national consistency and limit volatility between geographic areas.
Common Limitations and Criticisms
- Urban–Rural Misalignment: Many rural areas argue that their actual costs exceed GPCI-adjusted payments, particularly where labor or supply costs are rising faster than local indices.
- Data Lag: GPCI relies on multi-year cost surveys, which may not reflect current economic conditions or inflation trends.
- Limited Sensitivity: The model can underrepresent variation within large, diverse regions that share a single locality designation.
- Policy Constraints: Changes to GPCI often require congressional authorization, making reform slow and politically complex.
Relationship to Other Medicare Payment Factors
- GPCI interacts closely with the RBRVS structure and Medicare Conversion Factor, meaning shifts in one element can amplify or offset effects in another.
- In rural health contexts (e.g., RHCs or CAHs), GPCI has minimal or indirect influence, since those providers are reimbursed under cost-based methodologies like AIR (All-Inclusive Rate) rather than MPFS.
- GPCI reform is a recurring policy focus as CMS seeks to align regional fairness with sustainability for small and rural practices.
GPCI and Its Impact on Quality, Access, and Health Equity
The Geographic Practice Cost Index (GPCI) is one of Medicare’s primary mechanisms for regional payment equity, ensuring that reimbursement reflects the true cost of practicing medicine in different parts of the country. While its intent is to level the playing field, GPCI also shapes provider behavior, workforce distribution, and access to care—especially in rural, low-cost, and underserved regions.
Promoting Geographic Payment Fairness
- GPCI adjustments help equalize payment rates across regions, recognizing that operational costs differ dramatically between urban and rural practices.
- By indexing wages, rent, and malpractice premiums, GPCI prevents underpayment in high-cost areas, ensuring providers can maintain viable operations.
- This approach supports local economic alignment, allowing Medicare to fund care delivery that reflects real market conditions.
Influencing Workforce Distribution
- Higher GPCI-adjusted payments can make high-cost metropolitan regions financially attractive to physicians and specialists, helping offset higher living expenses.
- Conversely, providers in low-GPCI regions often face smaller reimbursements, which may discourage new clinicians from establishing rural or underserved practices.
- This imbalance has prompted policy efforts to stabilize rural payment rates through complementary programs such as HPSA incentives and RHC cost-based reimbursement (AIR).
Impact on Quality of Care and Access
- GPCI helps sustain quality by ensuring that resource-intensive regions are not underfunded, maintaining access to advanced technology and specialized services.
- However, low-GPCI regions may struggle to invest in infrastructure, leading to care access disparities, longer travel distances, and provider shortages.
- Over time, these payment differences can influence population health outcomes, particularly for chronic disease management in rural or low-income areas.
Challenges in Advancing True Equity
- GPCI’s reliance on broad geographic localities means some subregions—especially mixed urban–rural zones—do not receive accurately calibrated adjustments.
- The data lag in updating cost indices can delay reimbursement alignment with actual market inflation or housing cost spikes.
- Policymakers and industry experts have called for granular regional modeling or integration of social determinants of health (SDOH) to make future GPCI updates more equity-driven.
Evolving Toward a Fairer Payment Landscape
- CMS continues to refine GPCI methodology as part of a broader movement toward value-based and geographically balanced care models.
- Long-term equity may depend on blending GPCI adjustments with performance-based incentives that reward care quality and access rather than geography alone.
- Modernizing the GPCI framework is key to ensuring that regional fairness does not inadvertently perpetuate disparities in provider distribution or patient outcomes.
Frequently Asked Questions about the GPCI
1. What is the Geographic Practice Cost Index (GPCI)?
The GPCI is a Medicare payment adjustment factor that modifies physician reimbursement under the Medicare Physician Fee Schedule (MPFS) to account for regional cost differences. It ensures providers in higher-cost areas receive fair compensation for delivering the same services as those in lower-cost regions.
2. How is GPCI calculated?
The GPCI is based on three components of the Resource-Based Relative Value Scale (RBRVS):
- Work GPCI – Adjusts for physician labor costs.
- Practice Expense (PE) GPCI – Adjusts for office and overhead costs.
- Malpractice (MP) GPCI – Adjusts for regional liability insurance premiums.
Each GPCI value is derived from data collected by CMS and other federal agencies, such as the Bureau of Labor Statistics (BLS).
3. How does GPCI affect Medicare reimbursement?
Each CPT or HCPCS code’s total Relative Value Units (RVUs) are multiplied by the GPCI values specific to the provider’s locality. These adjusted RVUs are then multiplied by the Medicare Conversion Factor to determine the final payment.
Formula:
Payment = [(Work RVU × Work GPCI) + (PE RVU × PE GPCI) + (MP RVU × MP GPCI)] × Conversion Factor
4. How often is GPCI updated?
CMS reviews and updates GPCI data every three years, incorporating new wage and cost-of-living data from federal sources. Interim updates may occur when significant regional cost changes are identified or mandated by Congress.
5. What is the difference between GPCI and RVU?
- RVU (Relative Value Unit): Measures the relative resource cost of performing a service nationally.
- GPCI (Geographic Practice Cost Index): Adjusts those RVUs to reflect local cost variations.
Together, RVUs and GPCI determine the geographically adjusted total RVU, which is then converted to a dollar payment using the Conversion Factor.
6. How does GPCI differ from the All-Inclusive Rate (AIR)?
- GPCI applies to providers reimbursed under the MPFS, adjusting individual service payments based on geography.
- AIR (All-Inclusive Rate) applies to Rural Health Clinics (RHCs), which are reimbursed per encounter through a cost-based model rather than per service.
Both aim to promote fairness but operate under different reimbursement systems.
7. Why is GPCI important for healthcare equity?
GPCI ensures that providers in high-cost areas receive reimbursement that reflects the local cost of delivering care. However, it can also disadvantage rural and low-GPCI regions, where reimbursement rates may not keep pace with actual costs, contributing to provider shortages and access disparities.
