What is CC (Chief Complaint) in Healthcare?
CC (Chief Complaint) refers to the primary reason a patient seeks care, stated in their own words or summarized by the clinician at the beginning of a clinical encounter. The CC captures the patient’s immediate concern, symptom, or problem and serves as the entry point for clinical assessment and documentation.
In healthcare workflows, CC establishes the clinical focus of the encounter. It frames subsequent data collection, guides questioning, and helps clinicians prioritize evaluation. The CC is typically documented early—often during intake, triage, or SOC (Start of Care)—and appears prominently in clinical notes, assessments, and SOAP documentation.
Although the CC is brief, it has outsized importance. An accurate CC supports appropriate Dx (Diagnosis), informs the scope of evaluation, and helps justify why care was initiated. In Medicare-regulated and post-acute settings, CC documentation contributes to medical necessity by explaining the context for services provided.
Because CC anchors the clinical narrative, vague or generic chief complaints can weaken documentation, while clear and specific CC entries improve clarity, continuity, and compliance.
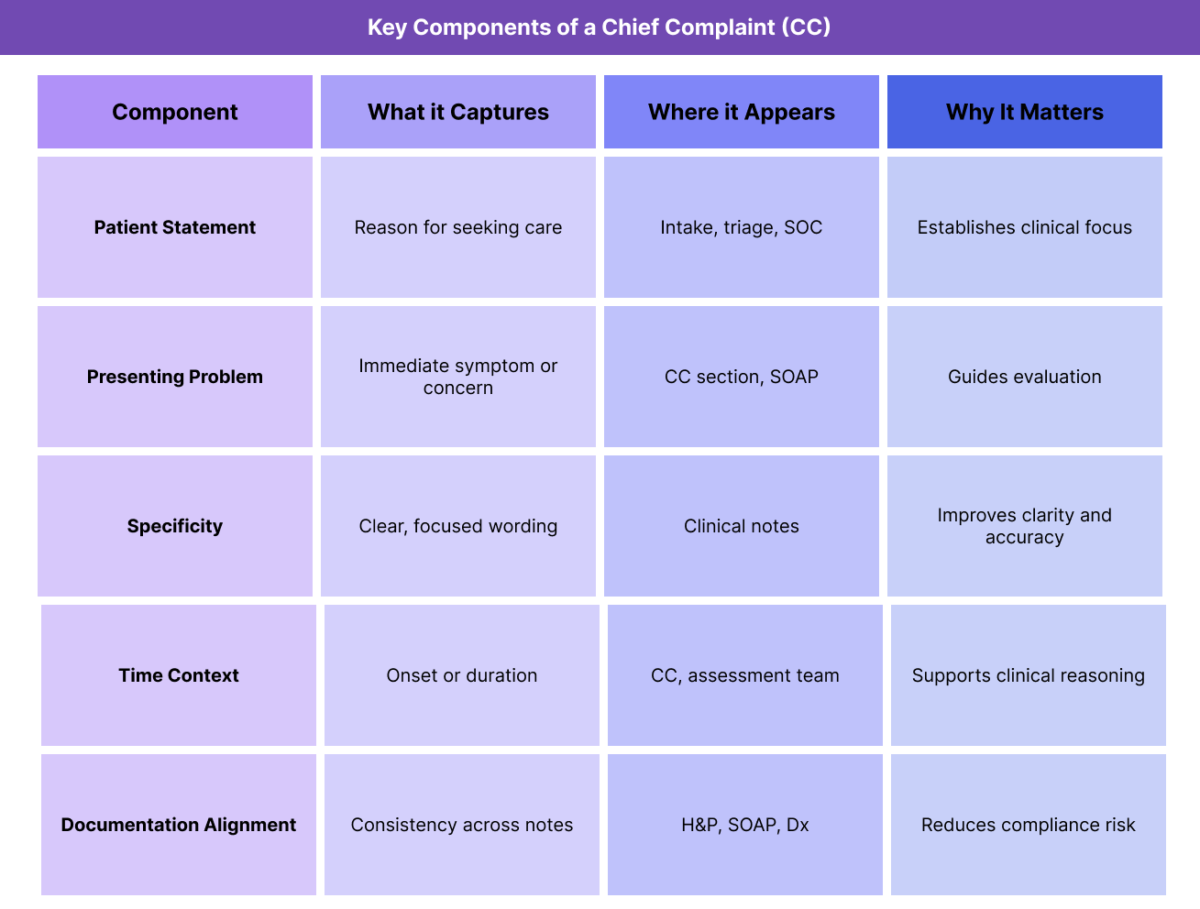
Key Components of a CC (Chief Complaint) in Healthcare
A well-documented CC contains several important characteristics that distinguish it from other clinical information.
Patient-Reported Concern
The CC is ideally stated in the patient’s own words whenever possible. This preserves accuracy and reflects the patient’s perspective, which is important for both clinical reasoning and documentation integrity.
Focus on the Presenting Problem
CC describes the current issue prompting care, not the full medical history. It is distinct from Hx (History), PMH (Past Medical History), or ROS (Review of Systems), which provide broader context.
Concise and Specific Language
Effective CC documentation is brief but specific. Clear wording helps clinicians quickly understand why the encounter occurred and what needs to be addressed first.
Temporal Context
Including duration or onset (e.g., “for three days,” “since discharge”) adds clinical value and supports assessment without turning the CC into a narrative history.
Consistency Across Documentation
The CC should align with later documentation, including the H&P (History and Physical), SOAP note, and assessment findings. Inconsistencies can raise questions during review.
How Chief Complaint (CC) Works in Practice
CC plays an active role throughout the clinical workflow, from initial contact through care planning.
Documenting CC During Intake and Start of Care (SOC)
The CC is often captured during intake or at SOC (Start of Care). Intake staff or clinicians document the patient’s stated concern, which becomes the anchor for the encounter.
In post-acute and home health settings, the CC often explains why services were initiated following a referral or transition.
Using CC to Guide Assessment and ROS
The CC directs the clinician’s assessment and informs which systems are reviewed during the ROS (Review of Systems). Rather than performing an unfocused evaluation, clinicians prioritize areas relevant to the CC.
This targeted approach improves efficiency and relevance.
CC Within SOAP and H&P Documentation
The CC appears prominently in SOAP notes and the H&P (History and Physical). It frames the subjective section and supports the assessment and plan that follow.
A clearly documented CC strengthens the clinical narrative across documentation formats.
Linking CC to Diagnosis (Dx)
The CC provides the starting point for clinical reasoning that leads to Dx (Diagnosis). While the CC is not itself a diagnosis, it explains why diagnostic evaluation occurred.
Alignment between CC and Dx is critical for medical necessity.
Referencing CC in Ongoing Care
Although CC is documented early, it continues to influence care decisions. Changes in the patient’s primary concern may prompt reassessment, updates to Tx (Treatment), or revisions to the care plan.
CC in Billing, Medical Necessity, and Documentation Oversight
Although the CC (Chief Complaint) is not billed directly, it plays a critical supporting role in how encounters are evaluated for medical necessity, documentation completeness, and audit readiness.
How CC Supports Medical Necessity
In Medicare-regulated and post-acute care settings, medical necessity depends on whether services are reasonable and necessary for the patient’s condition. The CC explains why care was initiated and provides context for the evaluation, assessment, and services that follow.
Reviewers often look at the CC alongside Dx (Diagnosis), Tx (Treatment), and the POC (Plan of Care) to determine whether the scope of care aligns with the patient’s stated concern. A vague or generic CC can weaken this narrative, even when care itself was appropriate.
CC and Documentation Integrity
The CC anchors the clinical story. Documentation reviewers expect the CC to logically connect to:
- Findings in the H&P (History and Physical)
- Symptoms addressed in the ROS (Review of Systems)
- The assessment and plan documented in SOAP notes
When the CC does not align with subsequent documentation, it raises questions about accuracy, completeness, or necessity.
CC as a Focus Area in Audits and Reviews
Auditors often evaluate whether:
- The CC reasonably justified the evaluation performed
- The CC aligns with the documented Dx
- Services delivered were appropriate given the CC
- Discrepancies between the CC and downstream documentation can trigger deeper review.
- Common CC-Related Documentation and Compliance Risks
Most CC-related issues stem from documentation habits rather than clinical intent.
Common risks include:
- Overly vague CC entries (e.g., “follow-up,” “check-up”)
- CC copied forward without updates
- CC not aligned with Dx or Tx
- CC missing temporal or symptom context
- Inconsistent CC wording across notes
Improving CC quality strengthens the entire documentation chain.
How CC Influences Quality, Access, and Equity
Beyond compliance, CC documentation affects patient experience and care equity.
CC and Quality of Care
A clear CC helps clinicians focus evaluation and treatment on what matters most to the patient. When the CC accurately reflects patient concerns, care is more targeted, efficient, and responsive.
Poorly documented CCs can lead to unfocused assessments or misaligned care priorities.
CC and Access to Services
The CC often determines whether an encounter is considered appropriate for care initiation or continuation, especially at SOC (Start of Care). Inadequate CC documentation can delay services or create barriers to enrollment.
Equity Considerations in Chief Complaint Documentation
Language barriers, health literacy differences, and cultural norms can affect how patients describe their concerns. Equity-aware CC documentation ensures the patient’s voice is accurately captured rather than oversimplified or misinterpreted.
Taking time to clarify and document CC appropriately helps reduce disparities in care.
Frequently Asked Questions about CC (Chief Complaint) in Healthcare
1. What does CC mean in healthcare?
CC stands for Chief Complaint and refers to the primary reason a patient seeks care. It captures the patient’s main concern or symptom and serves as the starting point for clinical evaluation, documentation, and care planning.
2. Is the chief complaint the same as a diagnosis?
No. The CC describes what the patient is experiencing or why they are seeking care, while Dx (Diagnosis) identifies the underlying condition based on assessment and evaluation. The CC leads to diagnostic reasoning but is not itself a diagnosis.
3. Where is the chief complaint documented?
The CC is typically documented during intake, triage, or at SOC and appears prominently in clinical notes, including SOAP documentation and the H&P. It often appears near the top of the medical record.
4. Why is the chief complaint important for documentation and audits?
The CC explains why care occurred. Auditors and reviewers use it to assess whether evaluations, services, and treatments were reasonable and necessary. A clear CC strengthens the documentation narrative and reduces compliance risk.
5. How detailed should a chief complaint be?
The CC should be concise but specific. It should clearly describe the patient’s primary concern without expanding into a full history. Additional detail belongs in the Hx, PMH, or ROS sections.
6. Can the chief complaint change during an episode of care?
Yes. While the CC is documented early, the patient’s primary concern may evolve. Significant changes should be reflected in updated documentation to maintain accuracy and relevance.
7. How does CC relate to SOC, Dx, and Tx?
The CC often explains why care begins at SOC, guides diagnostic evaluation (Dx), and shapes initial and ongoing treatment (Tx). Together, these elements form the clinical foundation of an episode of care.
