What is A/P (Assessment and Plan) in Healthcare?
A/P (Assessment and Plan) refers to the portion of clinical documentation where a clinician synthesizes available information about a patient’s condition and outlines the intended course of care. The A/P captures both the clinician’s clinical judgment (Assessment) and the specific actions to be taken (Plan).
In healthcare documentation, A/P is commonly used as shorthand to describe the final and most decision-oriented section of a clinical note. While A/P appears as part of SOAP documentation, it is often referenced independently in charts, progress notes, handoffs, and care summaries.
The Assessment portion reflects the clinician’s interpretation of subjective and objective findings and typically includes the working Dx (Diagnosis). The Plan portion translates that assessment into action, including Tx (Treatment) decisions, follow-up, education, and updates to the POC (Plan of Care).
Because A/P documents clinical reasoning and intent, it is one of the most scrutinized areas of the medical record. In Medicare-regulated and post-acute settings, the A/P is central to demonstrating medical necessity and appropriate care progression throughout the patient’s LOS (Length of Stay).
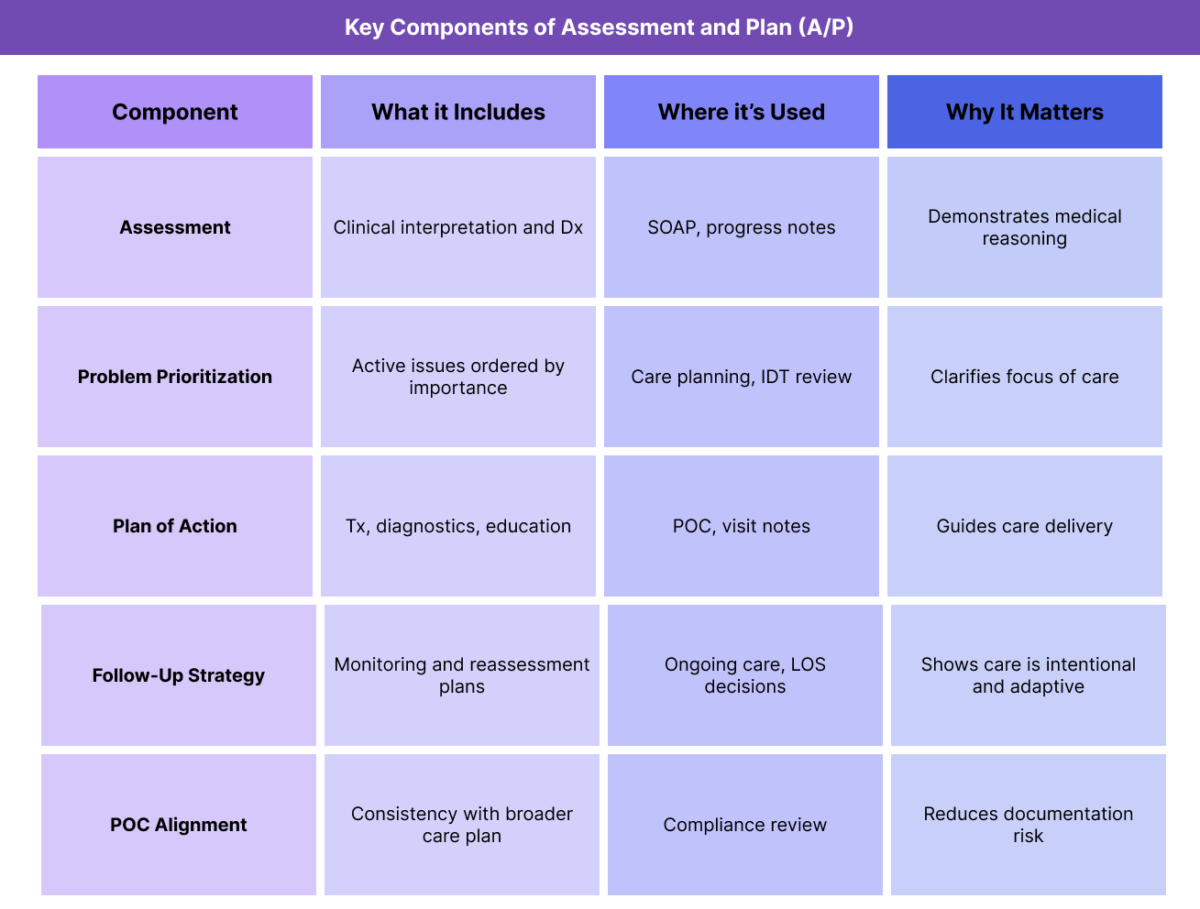
Key Components of the Assessment and Plan (A/P)
Although often brief in appearance, a high-quality A/P contains multiple distinct elements that together explain what the clinician believes is happening and what will be done next.
Clinical Assessment and Interpretation
The Assessment portion captures the clinician’s synthesis of patient-reported symptoms, exam findings, and relevant history. This is where the clinician explains their clinical judgment and documents Dx or diagnostic impressions.
A strong assessment goes beyond listing diagnoses—it explains relevance and prioritization.
Problem List and Prioritization
In many settings, the assessment is organized by problem, with each condition addressed separately. This structure clarifies clinical priorities and supports interdisciplinary understanding.
Treatment and Intervention Plan
The Plan outlines what actions will be taken to address the assessment. This may include medications, therapies, diagnostic testing, referrals, monitoring, and patient education.
Plans should be specific, actionable, and aligned with the documented assessment.
Follow-Up and Reassessment Strategy
A complete A/P includes plans for follow-up, reassessment, or criteria for modifying care. This demonstrates that care is dynamic and responsive to patient progress.
Alignment With the Plan of Care (POC)
The A/P should align with the broader POC (Plan of Care). Deviations should be clinically justified and documented to maintain consistency and compliance.
How Assessment and Plan (A/P) Works in Practice
A/P is used continuously throughout an episode of care to document decision-making and next steps.
Using A/P at Start of Care (SOC)
At SOC (Start of Care), the A/P captures initial clinical conclusions and establishes the direction of care. It explains why services are needed and how care will address the patient’s condition.
This initial A/P supports medical necessity and informs the POC.
Updating the A/P During Ongoing Care
As the patient progresses through their LOS (Length of Stay), the A/P is updated to reflect changes in condition, response to Tx, or new findings. These updates show that care decisions are based on current clinical information.
Static A/P entries across visits are a common audit concern.
A/P and Interdisciplinary Communication
The A/P is frequently referenced by the IDT (Interdisciplinary Team) to understand current priorities and planned actions. Clear A/P documentation supports coordinated care across disciplines.
Using A/P to Support Discharge Decisions
At DC (Discharge), the A/P helps explain why care is concluding and what follow-up actions are required. This supports continuity and compliance.
A/P in Billing, Medical Necessity, and Reimbursement Context
The A/P (Assessment and Plan) is one of the most important sections of the medical record when it comes to evaluating medical necessity, care appropriateness, and reimbursement integrity. Although A/P is not billed as a standalone service, it is frequently used by reviewers to understand why care was provided and what clinical decisions were made.
How A/P Supports Medical Necessity
Medical necessity requires more than documenting that care occurred—it requires demonstrating that care was reasonable and necessary for the patient’s condition. The A/P is where that justification is most clearly articulated.
A well-documented A/P explains:
- how the clinician interpreted the available data
- why a particular Dx (Diagnosis) is relevant and prioritized
- what Tx (Treatment) actions are appropriate in response
- how the care plan aligns with patient needs and risk
Reviewers often evaluate the A/P to determine whether services delivered during the patient’s LOS (Length of Stay) logically follow from the assessment documented at each encounter.
A/P and Reimbursement Integrity
Accurate A/P documentation helps ensure reimbursement reflects actual clinical decision-making. When the assessment clearly supports the plan, billed services are more likely to be viewed as appropriate and justified.
Common reimbursement issues arise when:
- the plan does not change despite documented improvement or decline
- treatments are continued without updated assessment
- the A/P does not align with the broader POC (Plan of Care)
These gaps can make care appear unnecessary or excessive during review.
Role of A/P in Episode-Based and Longitudinal Care Models
In episode-based and longitudinal models, the A/P functions as a decision log that explains how care evolved over time. Reviewers may examine successive A/P entries to assess whether care decisions were responsive to patient progress.
Strong A/P documentation shows that care was actively managed rather than passively continued.
Common A/P-Related Documentation and Compliance Risks
Because the A/P captures clinical judgment, it is a frequent focal point in audits and reviews.
Common risk patterns include:
- assessments that simply restate diagnoses without interpretation
- plans that list interventions without clinical rationale
- unchanged A/P language copied across visits
- mismatch between assessment findings and planned actions
- failure to document follow-up or reassessment criteria
These patterns can undermine the credibility of the medical record.
System and Workflow Challenges Affecting A/P Quality
The quality of A/P documentation is strongly influenced by documentation workflows and system design.
Over-Reliance on Templates
Templates can improve efficiency, but overly rigid templates often lead to generic A/P entries that do not reflect patient-specific reasoning. Auditors frequently flag templated assessments and plans that lack customization.
Fragmented Clinical Inputs
When subjective data, objective findings, and care actions are captured in different systems, clinicians may struggle to synthesize information effectively in the A/P.
Integrated workflows support clearer clinical reasoning.
Time Constraints and Cognitive Load
High documentation burden can lead clinicians to focus on task completion rather than narrative clarity. Without adequate support, A/P entries may omit important reasoning steps.
How A/P Influences Quality, Access, and Equity
Beyond compliance, the A/P has real-world implications for patient outcomes and care equity.
A/P and Quality of Care Outcomes
A clear A/P supports targeted, intentional care. When assessments are thoughtful and plans are specific, care is more likely to be effective and responsive to patient needs.
Poorly documented A/P entries can result in delayed adjustments to care or misaligned interventions.
A/P and Access to Healthcare Services
A/P documentation often supports decisions about whether care should continue, intensify, or conclude. Weak A/P documentation can delay authorizations, limit access to services, or result in premature discharge.
Equity Considerations in Assessment and Plan Documentation
Implicit bias, communication barriers, and incomplete history can influence assessment and planning. Equity-aware A/P documentation involves:
- grounding assessments in documented findings
- avoiding assumptions about patient behavior or compliance
- considering social and functional context documented in Hx (History) and PMH (Past Medical History)
Thoughtful A/P documentation helps ensure care decisions are fair and appropriate.
Frequently Asked Questions about A/P in Healthcare
1. What does A/P mean in healthcare?
A/P stands for Assessment and Plan and refers to the portion of clinical documentation where a clinician interprets patient information and outlines the intended course of care. It captures both clinical judgment and next steps.
2. How is A/P different from SOAP documentation?
A/P is a component of SOAP documentation, specifically representing the Assessment and Plan sections. While SOAP includes subjective and objective information, A/P focuses on interpretation and decision-making.
3. Why is A/P important for Medicare compliance?
In Medicare-regulated programs, the A/P demonstrates medical necessity by explaining why services are needed and how care decisions are based on patient condition. Reviewers often rely heavily on A/P documentation.
4. Should the A/P change at every visit?
The A/P should be reviewed and updated as the patient’s condition changes. While some elements may remain stable, unchanged A/P entries across visits are a common audit concern.
5. What happens if the assessment and plan do not align?
When the assessment does not logically support the plan, care may appear unnecessary or inappropriate. This misalignment increases compliance risk and can lead to denials or audits.
6. How does A/P relate to Dx, Tx, and the POC?
The assessment typically includes or refines Dx, while the plan outlines Tx actions and updates to the POC. Alignment across these elements strengthens documentation quality.
7. Can poor A/P documentation affect patient outcomes?
Yes. Incomplete or unclear A/P documentation can delay necessary care adjustments, reduce coordination across providers, and negatively affect outcomes.
