G3003 Description, Billing Rules, & Use Cases
HCPCS G3003 is the add-on code used to bill for each additional 15 minutes of Chronic Pain Management (CPM) personally delivered by a physician or other qualified healthcare professional (QHP) beyond the first 30 minutes in a calendar month.
This code is reported in addition to G3002 and is billable up to four units per calendar month under the CMS Medically Unlikely Edits (MUEs).
Like G3002, time billed under G3003 must be personally provided by the physician or QHP. It cannot be delegated to clinical staff or care coordinators.
What is HCPCS Code G3003?
HCPCS G3003 is the CMS code for each additional 15 minutes of CPM and treatment personally provided by a physician or QHP in a calendar month, after the first 30 minutes billed under G3002. The code was added by CMS effective January 1, 2023, and is always reported in addition to G3002.
The G3003 service is part of the same monthly CPM bundle as G3002, which includes:
- Diagnosis, assessment, and monitoring
- Administration of a validated pain rating scale or tool
- Development, implementation, revision, and maintenance of a person-centered care plan that includes strengths, goals, clinical needs, and desired outcomes
- Overall treatment management
- Medication management
- Pain and health literacy counseling
- Facilitation and coordination of any necessary behavioral health treatment
- Crisis care related to chronic pain when needed
- Ongoing communication and care coordination with other practitioners furnishing care, including physical therapy, occupational therapy, complementary and integrative approaches, and community-based care
G3003 should be used when:
- G3002 has been billed for the same patient in the same calendar month
- The provider personally delivers more than 30 minutes of CPM in the calendar month
- Each additional 15-minute increment of provider time is fully reached before the code is reported
- The patient meets all G3002 eligibility requirements, including an initial face-to-face visit of at least 30 minutes and documented consent in the medical record
- Time does not overlap with other care management codes for the same patient and same month
G3003 is capped at four units per calendar month per patient under the CMS Medically Unlikely Edits, with an MAI of 3 (date-of-service edit based on clinical benchmarks).
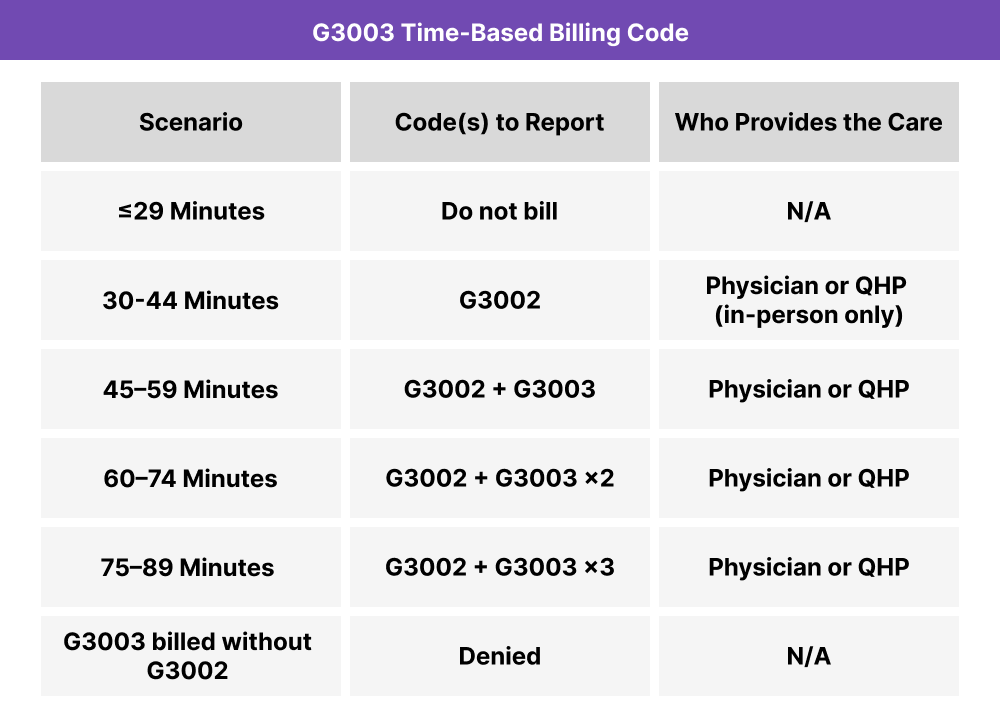
G3003 Time Thresholds and Code Combinations
G3003 is the add-on to G3002, reported only after each full 15-minute increment beyond the first 30 minutes is reached. Partial increments are not billable.
Important to Note:
G3003 cannot be billed without G3002 in the same calendar month. Only one practitioner can bill CPM for a given patient per month. CPM time cannot be reported alongside CCM, PCM, or APCM for the same patient in the same month, and time spent on those programs cannot be counted toward the G3003 increment.
When to Use G3003: Common Scenarios and Use Cases
G3003 is used when a physician or QHP has already met the 30-minute G3002 threshold in the calendar month and continues to personally deliver CPM services. Each additional 15-minute increment of documented time supports one unit of G3003.
Extended Care Plan Revision and Specialty Coordination
A physician spends the month:
- Conducting the initial G3002 monthly bundle work
- Coordinating with the patient’s neurologist and pain psychologist
- Revising the care plan to incorporate a new procedure recommendation
- Counseling the patient on expectations and recovery planning
Total qualifying time: 50 minutes
Billing: G3002 + G3003 x 1

Medication Transition and Behavioral Health Integration
A nurse practitioner delivers:
- Validated pain reassessment and care plan review
- Tapering plan for an opioid medication, coordinated with the patient’s behavioral health provider
- Multiple check-in calls to monitor symptoms and adjust the plan
- Care coordination notes with PT and the patient’s primary care provider
Total qualifying time: 65 minutes
Billing: G3002 + G3003 x 2

Complex Month With Crisis Care and Ongoing Coordination
A physician personally provides:
- The initial monthly bundle, including validated pain rating and care plan update
- Same-week crisis care for an acute pain flare, including medication review and ED coordination
- Follow-up calls and care plan revisions across the remainder of the month
- Coordination with PT, the patient’s behavioral health provider, and community-based care
Total qualifying time: 92 minutes
Billing: G3002 + G3003 x 4 (MUE cap)

G3003 Billing Requirements and Eligibility
G3003 carries the same patient, provider, and service requirements as G3002, plus the add-on rules as follows.
Patient Eligibility Criteria
- The patient is under the care of a Medicare-enrolled physician or other QHP
- The patient has a chronic pain condition that requires ongoing management
- The patient has received an initial face-to-face visit of at least 30 minutes from the billing physician or QHP
- Patient consent has been obtained and documented in the medical record, including that the patient has been informed about the service, applicable cost-sharing, the fact that only one practitioner can bill CPM per calendar month, and the patient’s right to stop services at any time
- G3002 has been billed for the same patient in the same calendar month
Provider Requirements
- The billing provider must be a physician or other QHP, including MDs, DOs, nurse practitioners, physician assistants, clinical nurse specialists, and certified nurse-midwives
- The provider must personally deliver each additional 15-minute increment of CPM in the calendar month
- Unlike Chronic Care Management (CCM) and Community Health Integration (CHI), time billed under G3003 cannot be delegated to auxiliary personnel, care coordinators, or community health workers
- The billing provider for G3003 must be the same practitioner who billed G3002 for that patient that month
Service Requirements
- Each 15-minute increment must be fully reached before the corresponding unit of G3003 can be billed
- G3003 may not be billed without a corresponding G3002 claim for the same patient and month
- A maximum of four units of G3003 may be billed per calendar month per patient under the CMS Medically Unlikely Edits
- All G3003 time must be part of the same person-centered care plan, validated pain rating, and monthly bundle activities reflected in the G3002 record
- Time must be distinct from time reported under other care management codes for the same patient and month
G3003 Billing Documentation Checklist
To compliantly bill G3003, your documentation must clearly show:
- A corresponding G3002 claim for the same patient in the same calendar month
- Each additional 15-minute increment of CPM personally performed by a physician or QHP, with specific dates and tasks recorded
- A running monthly time log that demonstrates each full 15-minute increment was reached before the unit was billed
- The same person-centered care plan referenced in the G3002 record, with any updates documented
- Notes reflecting the monthly bundle activities driving the additional time, such as:
- Extended medication management
- Multi-provider care coordination
- Behavioral health integration (BHI)
- Pain and health literacy counseling
- Crisis care, if delivered
- Communication with PT, OT, complementary and integrative providers, or community-based care
- A statement verifying that billed time is not duplicated or overlapped with CCM, PCM, APCM, BHI, TCM, or any other time-based care management code reported that month
- Confirmation that total billed G3003 units do not exceed four per calendar month per patient
Common G3003 Billing Mistakes (and How to Avoid Them)
❌ Writing off Denied G3003 Units Past the MUE
G3003 carries a Medically Unlikely Edit (MUE) of 4 with an MUE Adjudication Indicator (MAI) of 3; a clinical date-of-service edit, not an absolute one. Same-day units above 4 are denied, but unlike absolute edits, Medicare Administrative Contractors (MACs) may pay excess units on appeal or bypass the edit when medical necessity is documented. Treating every denial above the cap as final, rather than appealing with supporting documentation, leaves payable care unbilled.
❌ Billing G3003 Before a Full 15-Minute Increment is Reached
Each 15-minute increment must be fully met or exceeded. Documenting 12 or 14 minutes of additional time after the G3002 threshold is not sufficient. Round-up is not permitted.
❌ Counting Staff Time Toward G3003
G3003 time must be personally provided by the physician or QHP. Time spent by care coordinators, medical assistants, or community health workers does not count, even if the work supports the same care plan. This is the most significant operational difference between CPM and CCM.
❌ Billing More Than 4 Units of G3003 in a Calendar Month
The CMS Medically Unlikely Edits cap G3003 at 4 units per calendar month per patient, with an MAI of 3. Units beyond the cap are typically denied, and bypass requires documented medical necessity submitted on appeal.
❌ Two Practitioners Billing CPM for the Same Patient
Only one practitioner can bill CPM for a given patient per calendar month. If another provider in the practice or a referring provider has billed G3002 for the patient that month, G3003 cannot be reported by a second practitioner.
