What is SOAP (Subjective, Objective, Assessment, and Plan) in Healthcare?
SOAP is a structured documentation framework used by clinicians to record patient encounters in a clear, consistent, and clinically meaningful way. The acronym stands for Subjective, Objective, Assessment, and Plan, representing four distinct components of clinical reasoning and documentation.
In healthcare workflows, SOAP provides a standardized format for capturing patient-reported information, clinical findings, diagnostic interpretation, and care decisions. SOAP notes are widely used across care settings, including acute care, post-acute care, home health, and longitudinal Medicare programs.
SOAP documentation plays a critical role in care continuity, compliance, and audit readiness. Because SOAP notes clearly show how clinicians moved from patient concern to diagnosis and treatment, they are frequently reviewed by payers and regulators when evaluating medical necessity.
SOAP is not just a documentation preference—it is a clinical communication tool that helps ensure assessments are thorough, decisions are justified, and care plans are clearly articulated throughout the patient’s LOS (Length of Stay).
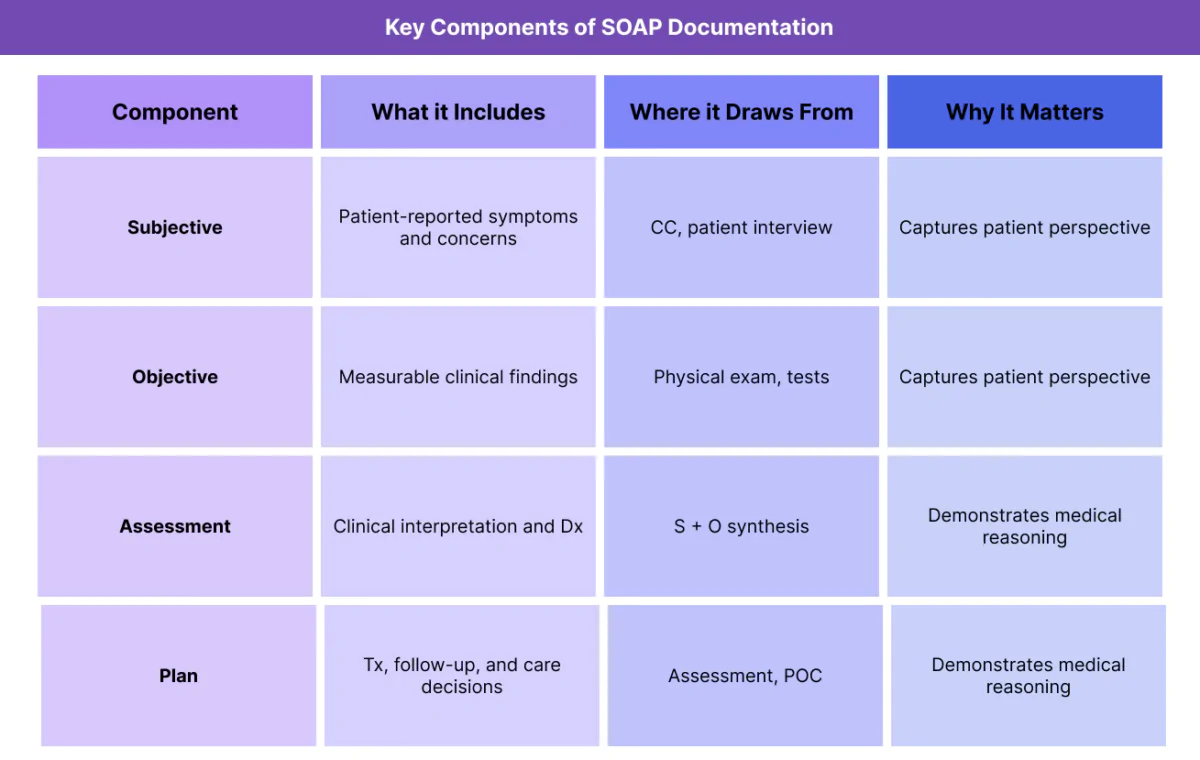
Key Components of the SOAP Framework
Each component of SOAP captures a different dimension of the patient encounter. Together, they form a complete clinical narrative.
Subjective (S)
The Subjective section captures information reported by the patient or caregiver. This includes the CC (Chief Complaint), symptom descriptions, patient concerns, and perceived changes since the last encounter.
Subjective information provides insight into the patient’s lived experience and often reflects changes that may not yet be visible in objective findings.
Objective (O)
The Objective section documents measurable and observable findings. This may include vital signs, physical exam results, lab values, imaging findings, or standardized assessment scores.
Objective data provides clinical evidence that supports—or challenges—subjective reports and helps ground the assessment in observable facts.
Assessment (A)
The Assessment represents the clinician’s interpretation of the subjective and objective information. This is where clinical reasoning occurs and where Dx (Diagnosis) is documented or refined.
The assessment explains what the clinician believes is happening and why.
Plan (P)
The Plan outlines the next steps in care. This includes Tx (Treatment) decisions, diagnostic testing, referrals, education, follow-up, and updates to the POC (Plan of Care).
The plan operationalizes the assessment into action.
How SOAP Works in Practice
SOAP is used repeatedly throughout an episode of care, not just at intake.
Using SOAP at Start of Care (SOC)
At SOC (Start of Care), SOAP notes help establish a baseline understanding of the patient’s condition. Subjective information captures why care began, while objective findings and assessment justify the need for skilled services.
This initial SOAP documentation supports medical necessity and care planning.
SOAP During Ongoing Care
Throughout the patient’s LOS (Length of Stay), SOAP notes document progress, setbacks, and changes in condition. Repeated SOAP documentation allows clinicians to show how the patient is responding to Tx and whether adjustments are needed.
Consistency across SOAP notes strengthens the clinical narrative.
SOAP and Interdisciplinary Communication
SOAP notes are commonly reviewed by the IDT (Interdisciplinary Team). A standardized SOAP format allows different disciplines to quickly understand patient status and coordinate care.
Using SOAP to Support Discharge (DC)
At DC (Discharge), SOAP documentation helps demonstrate that care goals were addressed and that discharge decisions were clinically appropriate.
SOAP in Billing, Medical Necessity, and Reimbursement Context
While SOAP documentation is not billed as a discrete service, it is one of the most heavily scrutinized forms of clinical documentation in Medicare-regulated and post-acute care environments. SOAP notes are frequently used by reviewers to evaluate whether services were reasonable, necessary, and appropriately delivered.
How SOAP Supports Medical Necessity
Medical necessity is evaluated by examining whether the care provided aligns logically with the patient’s condition and documented needs. SOAP notes demonstrate this alignment by showing the full chain of clinical reasoning:
- Subjective: what the patient reports and experiences
- Objective: what the clinician observes and measures
- Assessment: how the clinician interprets that information and determines Dx (Diagnosis)
- Plan: what actions are taken in response, including Tx (Treatment) and updates to the POC (Plan of Care)
When SOAP notes are complete and internally consistent, they clearly show why services were delivered and how decisions were made throughout the patient’s LOS (Length of Stay).
SOAP and Reimbursement Integrity
Accurate SOAP documentation helps ensure reimbursement reflects actual care delivered. SOAP notes are often reviewed alongside billing data to confirm that:
- services billed were actually provided
- visit frequency aligns with patient needs
- Tx intensity is supported by documented findings
Incomplete or generic SOAP notes can make care appear unsupported, even when services were appropriate, increasing the risk of denials or recoupment.
SOAP in Episode-Based and Longitudinal Care Models
In episode-based and longitudinal models, SOAP notes collectively tell the story of the episode from SOC (Start of Care) through DC (Discharge). Reviewers may evaluate SOAP documentation to assess:
- whether patient progress justified continued care
- whether changes in condition were addressed appropriately
- whether discharge timing aligned with documented improvement
SOAP consistency across visits is especially important in these models.
Common SOAP-Related Documentation and Compliance Risks
SOAP-related compliance risk most often stems from documentation habits rather than clinical decision-making.
Common risk patterns include:
- Copy-forward SOAP notes without updates
- Subjective sections that repeat unchanged language across visits
- Objective findings that do not support the assessment
- Assessment sections that simply restate Dx without interpretation
- Plans that do not change despite patient improvement or decline
Auditors frequently identify these patterns as indicators of poor documentation quality.
System and Workflow Challenges Affecting SOAP Quality
SOAP documentation quality is heavily influenced by how systems and workflows are designed.
Over-Templating and Automation Risks
Templates improve efficiency, but excessive templating can lead to repetitive, non-specific SOAP notes. Automated text that is not customized to the patient’s condition weakens credibility and increases audit risk.
Fragmented Data Inputs
When subjective reports, objective data, and treatment actions are captured in separate systems, clinicians may struggle to synthesize information effectively within the SOAP structure.
Limited Time for Documentation
Time pressure can lead clinicians to prioritize speed over detail. Without structured prompts or safeguards, SOAP notes may omit critical reasoning steps that reviewers expect to see.
How SOAP Influences Quality, Access, and Equity
SOAP documentation affects more than compliance—it shapes care quality and fairness.
SOAP and Quality of Care Outcomes
High-quality SOAP documentation supports accurate Dx, targeted Tx, and timely adjustments to care plans. When clinicians clearly document reasoning and response to care, outcomes tend to improve.
Poor SOAP documentation can obscure patient progress or delay needed changes in treatment.
SOAP and Access to Healthcare Services
SOAP notes often support decisions about whether care should continue, intensify, or conclude. Inadequate documentation can delay approvals, limit access to services, or result in premature discharge.
Equity Considerations in SOAP Documentation
Patient-reported information in the Subjective section may be influenced by language barriers, cultural norms, or health literacy. Equity-aware SOAP practices involve clarifying patient statements, avoiding assumptions, and documenting context accurately.
Objective findings and assessments should be interpreted with awareness of social and functional factors documented in Hx (History) and PMH (Past Medical History).
Frequently Asked Questions about SOAP in Healthcare
1. What does SOAP mean in healthcare?
SOAP stands for Subjective, Objective, Assessment, and Plan. It is a standardized format for documenting patient encounters that captures patient-reported information, clinical findings, diagnostic interpretation, and care decisions.
2. Why is SOAP documentation important for Medicare compliance?
In Medicare-regulated programs, SOAP notes demonstrate medical necessity by showing how clinical decisions were made. Reviewers often rely on SOAP documentation to determine whether services were appropriate and supported throughout the episode of care.
3. How is SOAP different from the H&P?
The H&P (History and Physical) establishes a comprehensive baseline at the beginning of care, while SOAP notes are typically used for ongoing, visit-level documentation. Findings from the H&P inform SOAP documentation, but the two serve different purposes.
4. Do SOAP notes need to change at every visit?
Yes. While some elements may remain stable, SOAP notes should reflect changes in patient condition, response to Tx, or progress toward goals. Identical notes across visits are a common audit concern.
5. What happens if SOAP documentation is incomplete or inconsistent?
Incomplete or inconsistent SOAP documentation can weaken medical necessity justification, increase audit risk, and lead to delayed or denied payment—even when care was clinically appropriate.
6. How does SOAP relate to CC, ROS, Dx, and Tx?
SOAP integrates information from the CC (Chief Complaint) and ROS (Review of Systems) into an assessment that informs Dx (Diagnosis) and guides Tx (Treatment). Consistency across these elements strengthens documentation quality.
7. Can poor SOAP documentation affect patient outcomes?
Yes. Poor documentation can obscure changes in condition, delay necessary adjustments to care, and reduce continuity across providers, negatively affecting outcomes and experience.
