What is ROS (Review of Systems) in Healthcare?
ROS (Review of Systems) is a structured method of systematically questioning a patient about symptoms related to major body systems. The purpose of the ROS is to identify current symptoms, uncover previously unreported issues, and provide clinical context for assessment and diagnosis.
In healthcare documentation, ROS expands upon the CC (Chief Complaint) by exploring related and unrelated symptoms across multiple systems. While the CC captures why the patient is seeking care, the ROS helps clinicians understand the broader clinical picture that may influence Dx (Diagnosis), Tx (Treatment), and care planning.
ROS is commonly documented during intake, assessment, or at SOC (Start of Care) and appears prominently in SOAP notes and the H&P (History and Physical). In Medicare-regulated and post-acute settings, ROS contributes to medical necessity by demonstrating a thorough and appropriate clinical evaluation.
Although ROS is often standardized, its quality depends on relevance and accuracy. A well-performed ROS supports clinical reasoning, while an unfocused or copied ROS can weaken documentation and increase audit risk.
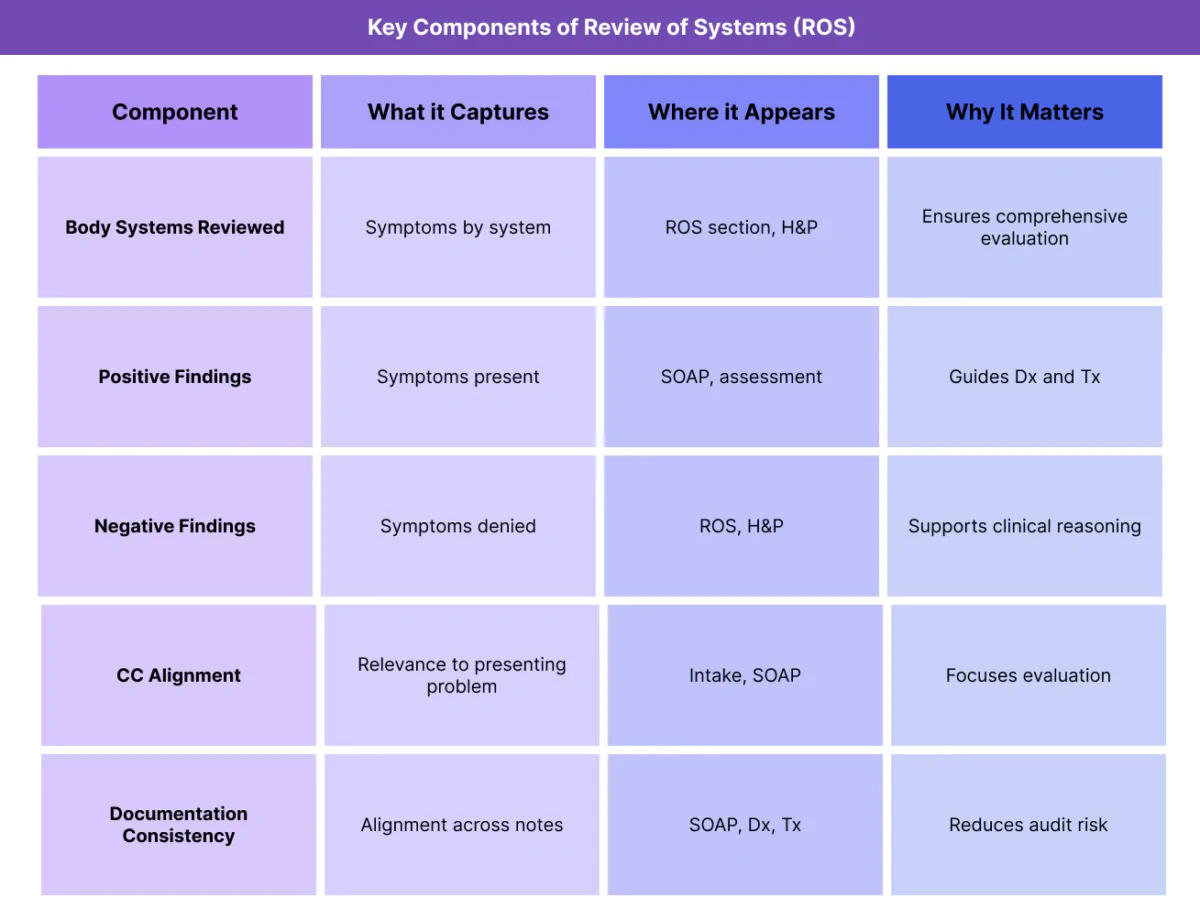
Key Components of the ROS (Review of Systems) in Healthcare
The ROS is organized by body systems, allowing clinicians to capture symptoms in a consistent and comprehensive way.
System-Based Symptom Review
ROS evaluates symptoms across systems such as cardiovascular, respiratory, gastrointestinal, neurological, musculoskeletal, and others. Each system is addressed to determine the presence or absence of relevant symptoms.
Positive and Negative Findings
ROS documentation includes both positive findings (symptoms present) and pertinent negatives (symptoms denied). Documenting negatives helps rule out conditions and supports diagnostic reasoning.
Relevance to the Chief Complaint (CC)
An effective ROS prioritizes systems related to the CC (Chief Complaint) while still screening for broader issues that may affect care.
Patient-Reported Information
ROS relies primarily on patient-reported symptoms, making clear communication and clarification essential—especially when patients have difficulty describing symptoms.
Consistency Across Documentation
ROS findings should align with information in the Hx (History), PMH (Past Medical History), physical exam, and assessment sections. Inconsistencies can raise documentation concerns.
How Review of Systems (ROS) Works in Practice
ROS is an active part of the clinical workflow, supporting evaluation and decision-making throughout care.
Performing ROS During Intake and Start of Care (SOC)
ROS is often conducted during intake or at SOC (Start of Care). Clinicians ask structured questions to identify symptoms that may influence assessment and care planning.
In post-acute settings, ROS helps validate the need for services following referral or discharge from another setting.
Using ROS to Support Diagnosis (Dx)
ROS findings provide critical context for Dx (Diagnosis). Positive symptoms help narrow diagnostic possibilities, while negative findings help rule out conditions.
A well-documented ROS strengthens diagnostic justification.
ROS Within SOAP Documentation
In SOAP notes, ROS findings typically appear in the subjective section and inform the assessment and plan. ROS bridges the patient’s reported experience with clinical interpretation.
Integrating ROS With History and Physical Exam
ROS complements Hx (History), PMH, and the physical exam. Together, these elements create a comprehensive picture of the patient’s condition.
Fragmented ROS documentation weakens this narrative.
Updating ROS Over Time
While ROS is commonly documented early, it may be updated if symptoms change during the patient’s LOS (Length of Stay). Updated ROS findings help ensure ongoing care remains appropriate.
ROS in Billing, Medical Necessity, and Documentation Oversight
The ROS (Review of Systems) is not billed as a standalone service, but it plays an important supporting role in demonstrating the appropriateness and completeness of a clinical evaluation.
How ROS Supports Medical Necessity
In Medicare-regulated and post-acute care settings, medical necessity depends on whether the evaluation performed was reasonable given the patient’s CC (Chief Complaint) and clinical context. ROS documentation helps show that clinicians appropriately explored symptoms related to the presenting concern.
Reviewers often assess whether the depth and scope of ROS align with the complexity of the patient’s condition and the services provided under the POC (Plan of Care).
ROS and Documentation Integrity
ROS serves as a bridge between subjective patient reporting and clinical assessment. Documentation reviewers expect ROS findings to logically connect to:
- The H&P (History and Physical)
- Assessment and plan sections in SOAP notes
- The resulting Dx (Diagnosis)
When ROS documentation is copied forward or inconsistent, it can undermine credibility.
ROS as an Audit and Review Focus Area
Auditors may evaluate whether:
- ROS scope was appropriate for the encounter
- ROS findings support the Dx
- Positive and negative findings were documented consistently
Generic or templated ROS entries are common audit concerns.
Common ROS-Related Documentation and Compliance Risks
Most ROS-related issues arise from documentation practices rather than clinical judgment.
Common risks include:
- ROS copied forward without updates
- ROS that does not align with CC
- Missing pertinent negatives
- Inconsistencies between ROS and physical exam
- Overly extensive ROS unrelated to the encounter
Improving ROS relevance strengthens documentation quality.
How ROS Influences Quality, Access, and Equity
ROS affects patient experience and care equity.
ROS and Quality of Care
A focused ROS helps clinicians identify symptoms that may otherwise be overlooked. This supports accurate Dx and appropriate Tx, improving overall care quality.
ROS and Access to Healthcare Services
Clear ROS documentation supports timely care decisions and reduces delays caused by incomplete assessments, particularly at SOC (Start of Care).
Equity Considerations in Review of Systems
Language barriers, cultural norms, and health literacy differences can affect how patients describe symptoms. Equity-aware ROS practices ensure that patient-reported information is accurately captured and interpreted.
Clarifying symptoms and using appropriate communication methods helps reduce disparities.
Frequently Asked Questions about ROS) in Healthcare
1. What does ROS mean in healthcare?
ROS stands for Review of Systems and refers to a structured process of asking a patient about symptoms across major body systems. It helps clinicians identify relevant symptoms and provides context for diagnosis and care planning.
2. How is ROS different from the chief complaint?
The CC (Chief Complaint) captures the patient’s main reason for seeking care, while the ROS explores additional symptoms across body systems. Together, they provide a more complete picture of the patient’s condition.
3. Is ROS required for every patient encounter?
ROS is commonly documented during comprehensive evaluations, such as intake, SOC, or initial assessments. The extent of ROS should be appropriate to the encounter and the patient’s condition.
4. Where is ROS documented in clinical notes?
ROS is typically documented in the subjective section of SOAP notes and in the H&P. It may also appear in structured assessment forms.
5. Can ROS change during an episode of care?
Yes. Symptoms may evolve over time. When changes occur, ROS documentation should be updated to reflect the patient’s current status and support ongoing care decisions.
6. Why is ROS important for audits and compliance?
ROS demonstrates that an appropriate evaluation was performed. Inadequate or generic ROS documentation can raise questions about medical necessity and documentation quality.
7. How does ROS relate to Dx, Tx, and the POC?
ROS findings inform Dx by identifying relevant symptoms, guide Tx decisions, and support the POC by demonstrating clinical need. Consistency across these elements strengthens documentation.
