What is ADL (Activities of Daily Living) in Healthcare?
ADLs (Activities of Daily Living) refer to the basic self-care tasks that individuals must be able to perform in order to live independently and safely. ADLs are a core measure of functional status and are widely used in clinical assessment, care planning, and discharge decision-making across healthcare settings.
In healthcare, ADLs provide practical insight into how a patient’s health conditions affect day-to-day functioning. Limitations in ADLs often signal the need for clinical intervention, supportive services, or ongoing care. ADL status is particularly important in post-acute, home health, and Medicare-regulated programs, where functional ability is closely tied to eligibility, care intensity, and outcomes.
ADLs are commonly assessed at SOC (Start of Care) and revisited throughout the patient’s LOS (Length of Stay) to track progress and inform Tx (Treatment) decisions. Changes in ADL performance frequently influence Dx (Diagnosis) refinement, updates to the POC (Plan of Care), and readiness for DC (Discharge).
Because ADLs directly reflect a patient’s ability to function in daily life, accurate assessment and documentation are critical to both care quality and compliance.
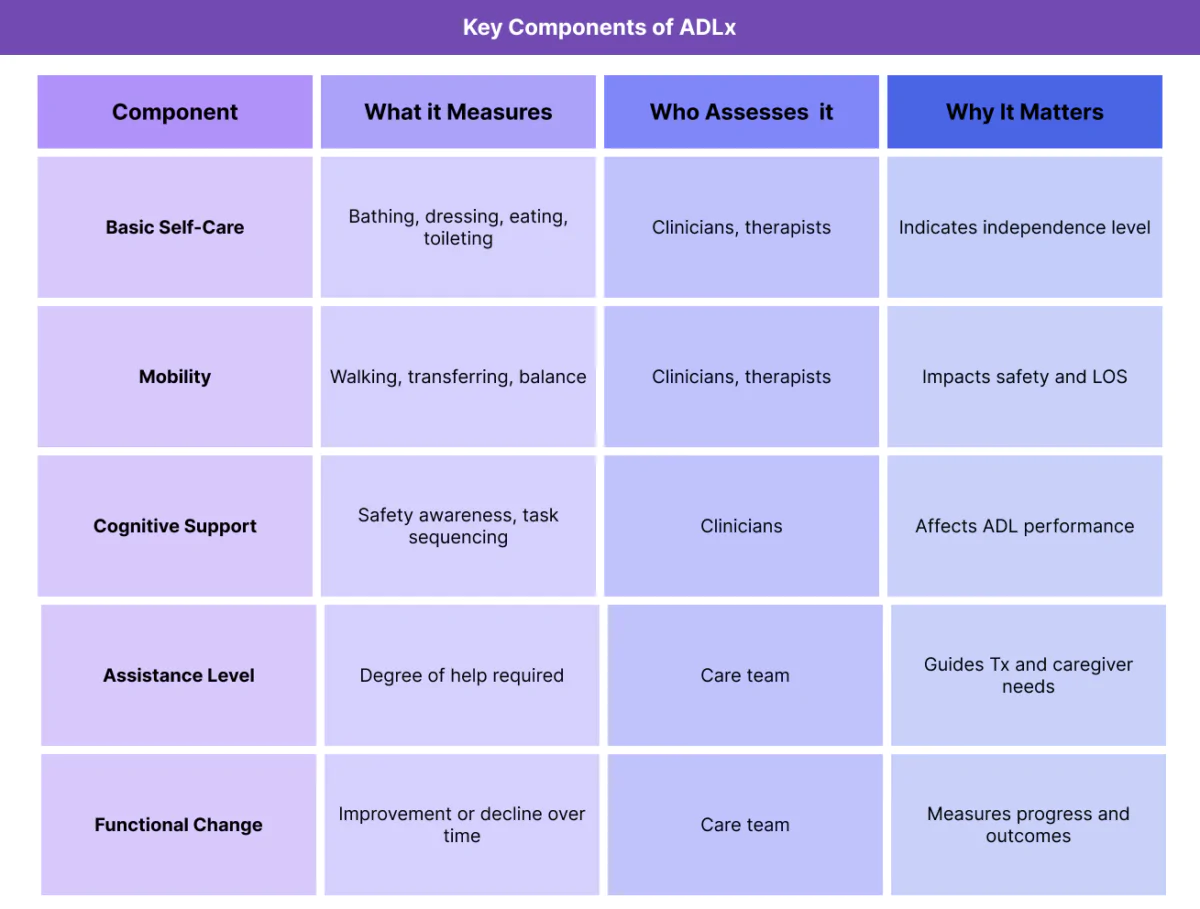
Key Components of ADL in Healthcare
ADLs are typically grouped into specific categories that capture different aspects of daily self-care.
Basic Self-Care Activities
Basic ADLs include essential personal care tasks such as bathing, dressing, eating, toileting, and transferring. These activities are foundational to independent living and are commonly evaluated during initial assessments.
Limitations in basic ADLs often indicate the need for skilled services or caregiver support.
Mobility and Functional Movement
Mobility-related ADLs assess a patient’s ability to move safely, including walking, transferring between positions, and maintaining balance. Mobility limitations can significantly increase fall risk and affect LOS.
Cognitive and Safety-Related Functioning
While ADLs primarily focus on physical tasks, cognitive ability and safety awareness are closely linked. Patients may be physically capable but unable to perform ADLs safely due to cognitive impairment.
Level of Assistance Required
ADL assessment evaluates not only whether a patient can perform a task, but how much assistance is required—ranging from independent to total dependence. This distinction is critical for care planning.
Change Over Time
ADL status is dynamic. Improvement or decline over time provides insight into treatment effectiveness and informs ongoing care decisions.
How ADLs Work in Practice
ADLs are used throughout the care episode to guide clinical and operational decisions.
Assessing ADLs at Start of Care (SOC)
ADL assessment is typically performed at SOC (Start of Care) to establish a functional baseline. Clinicians evaluate which activities the patient can perform independently and where assistance is required.
This baseline informs initial Dx (Diagnosis) context and supports development of the POC (Plan of Care).
Using ADLs to Guide Treatment (Tx)
ADL limitations directly influence Tx (Treatment) selection. Therapy services, nursing interventions, and education are often designed to improve or maintain ADL function.
Tx progress is frequently measured by changes in ADL performance.
Monitoring ADL Progress During LOS
Throughout the patient’s LOS (Length of Stay), clinicians reassess ADLs to track improvement or decline. These changes help determine whether Tx remains effective or requires adjustment.
Consistent ADL tracking supports medical necessity documentation.
Coordinating ADL Support Across the IDT
ADL-related needs often require collaboration across the IDT (Interdisciplinary Team). Therapists, nurses, and care coordinators contribute different perspectives on functional status and support needs.
Shared understanding of ADL status reduces fragmented care.
Using ADLs to Determine Discharge Readiness
At DC (Discharge), ADL performance is a key indicator of readiness. Patients must be able to safely perform essential activities or have appropriate support in place.
ADL status frequently determines whether discharge is appropriate or whether additional services are needed.
ADLs in Billing, Medical Necessity, and Reimbursement
While ADLs are not billed as standalone services, they play a critical supporting role in determining medical necessity, care eligibility, and reimbursement—particularly in Medicare-regulated and post-acute care programs.
How ADLs Support Medical Necessity
In Medicare programs, medical necessity is evaluated based on a patient’s functional limitations and need for skilled services. Documented ADL impairments help explain why care is required and what type of services are appropriate.
When ADL limitations are clearly documented, they support:
- Skilled therapy or nursing need
- Ongoing Tx (Treatment) during the LOS (Length of Stay)
- Continued services under the POC (Plan of Care)
Without documented ADL deficits, payers may question whether skilled care is justified.
ADLs and Reimbursement Integrity
ADL documentation helps ensure reimbursement aligns with patient complexity and care intensity. Functional limitations often explain why patients require more frequent visits, longer LOS, or interdisciplinary involvement.
Understated ADL limitations can lead to underpayment, while exaggerated or unsupported ADL deficits increase audit risk.
ADLs in Episode-Based and Post-Acute Care Models
In episode-based and post-acute models, ADLs are often used to assess baseline function and track progress. Payers may compare functional improvement against expected outcomes based on documented ADL status.
Lack of improvement without documented clinical justification can trigger review.
Common ADL-Related Documentation and Compliance Risks
ADL-related compliance issues usually stem from inconsistent or incomplete documentation rather than improper care.
Common risks include:
- ADL assessments not completed at SOC (Start of Care)
- Inconsistent ADL documentation across visits
- Failure to document changes in ADL status
- ADL limitations not aligned with Dx (Diagnosis) or Tx
- Missing ADL context at DC (Discharge)
Auditors frequently review ADL documentation when evaluating necessity and outcomes.
System and Workflow Challenges Affecting ADL Documentation
Accurate ADL documentation depends heavily on workflow design and system support.
Fragmented ADL Data Collection
When ADL information is scattered across notes or systems, it becomes difficult to demonstrate progress or justify ongoing care.
Infrequent Reassessment of ADLs
ADLs should be reassessed throughout LOS, not only at SOC and DC. Failure to update ADL status can weaken documentation and clinical decision-making.
Limited IDT Visibility Into ADL Status
If ADL information is not easily accessible to the IDT (Interdisciplinary Team), care planning and coordination suffer.
How ADLs Influence Quality, Access, and Equity
ADLs have a direct impact on patient outcomes and fairness in care delivery.
ADLs and Quality of Care Outcomes
Improvement or stabilization in ADLs is often a primary goal of post-acute care. Accurate ADL assessment helps clinicians tailor Tx and measure meaningful progress.
ADLs and Access to Healthcare Services
ADL limitations often determine eligibility for services and level of support. Inadequate documentation can delay access to needed care or result in inappropriate discharge.
Equity Considerations in ADL Assessment
Cultural norms, language barriers, and social context can influence how ADL ability is reported and assessed. Equity-aware ADL evaluation ensures that functional limitations are accurately understood and addressed.
Failure to account for these factors can lead to disparities in care planning and outcomes.
Frequently Asked Questions about ADLs in Healthcare
1. What are ADLs in healthcare?
ADLs, or Activities of Daily Living, are basic self-care tasks such as bathing, dressing, eating, toileting, and mobility. In healthcare, ADLs are used to assess a patient’s functional ability and need for care or support.
2. Why are ADLs important in Medicare programs?
Medicare programs use ADL limitations to help determine medical necessity, care eligibility, and appropriate service intensity. Documented ADL impairments support the need for skilled services and ongoing Tx.
3. How are ADLs assessed in post-acute care?
ADLs are assessed through clinician observation, patient interview, and standardized assessment tools, often at SOC and reassessed throughout LOS to track progress.
4. Can ADL status change during an episode of care?
Yes. ADL performance often improves or declines over time. Changes in ADL status should be documented to reflect patient progress and support ongoing care decisions.
5. How do ADLs affect discharge planning?
At DC, ADL performance helps determine whether a patient can safely return home, requires caregiver support, or needs additional services. ADL status is a key indicator of discharge readiness.
6. Are ADLs the same as IADLs?
No. ADLs refer to basic self-care tasks, while IADLs (Instrumental Activities of Daily Living) involve more complex activities such as managing finances, cooking, or transportation. Both provide insight into functional ability but serve different roles in assessment.
7. Can poor ADL documentation affect audits or payment?
Yes. Inconsistent or missing ADL documentation can weaken medical necessity justification and increase audit risk, even when care was clinically appropriate.
