What is STEMI (ST-Elevation Myocardial Infarction) in Healthcare?
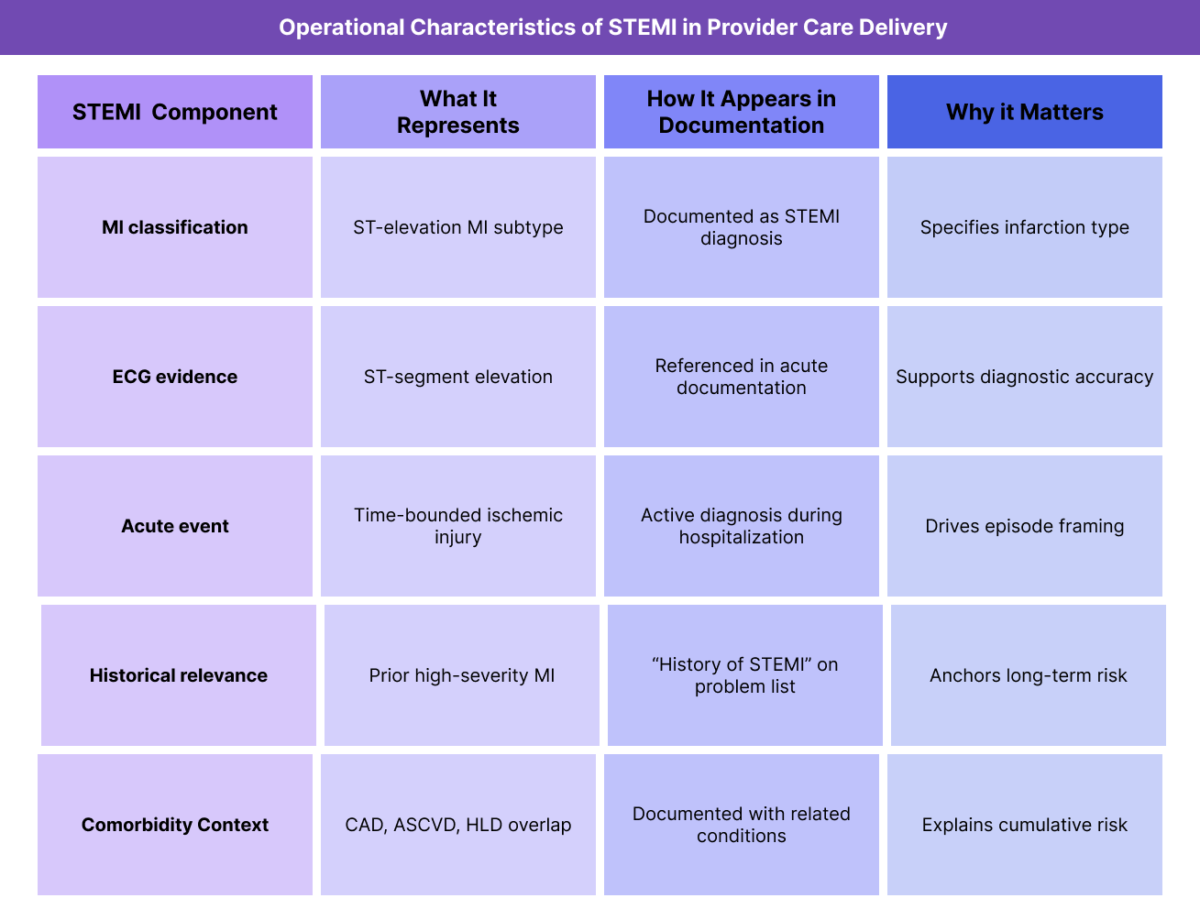
STEMI (ST-Elevation Myocardial Infarction) is a classification of MI (Myocardial Infarction) characterized by evidence of acute myocardial injury accompanied by ST-segment elevation on an ECG (also referred to as EKG). In healthcare documentation and provider workflows, STEMI represents a specific type of acute MI event, not a chronic diagnosis.
From a B2B and operational standpoint, STEMI is documented to establish that a patient experienced a high-severity ischemic cardiac event with clear diagnostic criteria. While STEMI itself is time-bounded, its occurrence has long-term relevance for risk stratification, problem list management, and longitudinal care planning.
In Medicare and adult populations, STEMI commonly appears in records as:
- an acute inpatient diagnosis, and later
- a historical event (e.g., “history of STEMI”)
STEMI documentation is particularly important because it conveys event severity and helps distinguish the infarction type when compared to other MI classifications such as NSTEMI. This distinction affects how prior cardiac injury is interpreted in downstream care.
Operationally, STEMI functions as an event marker that anchors cardiovascular risk narratives alongside related conditions such as CAD, ASCVD, CHF, HLD, and CKD.
Key Clinical and Operational Components of STEMI in Healthcare
STEMI’s significance lies in its role as a clearly defined MI subtype with implications for documentation accuracy, longitudinal risk context, and care coordination.
STEMI as a Classification of MI
STEMI is not a standalone disease; it is a classification within the broader MI diagnosis. Providers document STEMI to specify the type of myocardial infarction that occurred, based on ECG findings and clinical criteria.
This classification improves clarity and reduces ambiguity in the medical record.
STEMI and ECG (EKG) Documentation Context
STEMI is defined in part by ST-segment elevation identified on an ECG (EKG). In provider documentation, ECG findings are referenced to support the STEMI classification, but interpretation details are typically not restated in longitudinal notes.
Operationally, ECG context supports the accuracy of the initial STEMI diagnosis.
STEMI as an Acute Event With Long-Term Relevance
While STEMI is an acute event, it remains relevant long after resolution. Providers often document STEMI history to explain:
- elevated cardiovascular risk
- secondary prevention strategies
- ongoing monitoring decisions
This dual acute-historical nature makes clear documentation especially important.
STEMI in Diagnosis and Problem List Management
During the acute phase, STEMI is documented as an active diagnosis. After resolution, it is typically transitioned to history of STEMI on the problem list.
Clear differentiation between active and historical status supports accurate longitudinal records.
STEMI and Comorbidity Interaction
STEMI frequently occurs in patients with underlying CAD, ASCVD, HTN, HLD, CKD, or AFib. Providers document STEMI to explain how acute ischemic injury compounds existing cardiovascular disease burden.
This interaction supports comprehensive risk narratives.
How STEMI Is Documented and Used in Practice
STEMI documentation changes over time as the patient moves from acute care to longitudinal management.
STEMI During the Acute Care Episode
During the acute episode, STEMI documentation focuses on:
- confirmation of MI type
- ECG findings supporting classification
- timing and sequencing of the event
- associated diagnoses and interventions
Precision during this phase is critical for downstream documentation integrity.
STEMI as History in Longitudinal Care
After resolution, STEMI is documented as a historical event rather than an active condition. Providers reference prior STEMI to support risk stratification, monitoring decisions, and care planning.
Accurate dating and status labeling reduce confusion in longitudinal records.
STEMI and Interdisciplinary Communication
Clear STEMI documentation helps the IDT understand the severity and implications of prior cardiac injury. This shared understanding supports coordinated care and consistent risk assessment across settings.
STEMI in Transitions of Care
STEMI history is especially important during transitions of care, where clarity about prior cardiac events helps receiving providers contextualize current status and risk.
STEMI in Billing, Reimbursement, and System Limitations
How STEMI Supports Medical Necessity Documentation
STEMI (ST-Elevation Myocardial Infarction) represents a clearly defined acute ischemic cardiac event with objective diagnostic criteria. In billing and reimbursement review, STEMI documentation establishes high-severity medical necessity during the acute episode and provides enduring context for post-event care.
Although STEMI itself is time-limited, accurate documentation confirms that myocardial injury occurred, which justifies downstream monitoring, secondary prevention, and coordinated follow-up after discharge.
STEMI and Acute Episode Framing
From a reimbursement perspective, STEMI documentation is closely tied to episode framing. Clear identification of STEMI as an acute MI subtype helps define:
- the start of the acute cardiac episode
- the severity of the presenting condition
- the intensity of services delivered
Precise STEMI documentation reduces ambiguity when distinguishing acute care from post-acute or longitudinal management.
STEMI as Historical Context After Resolution
Once the acute event has resolved, STEMI should be documented as history of STEMI rather than an active diagnosis. In this historical context, STEMI supports medical necessity by explaining why patients remain at elevated cardiovascular risk despite clinical stability.
This distinction is critical to avoid misclassification during reimbursement review.
Reimbursement Risk When STEMI Is Poorly Documented
STEMI documentation can create reimbursement risk when:
- acute status is carried forward indefinitely
- event timing is unclear or omitted
- STEMI is documented without confirmation of MI
- historical STEMI is conflated with active ischemia
Clear transition from acute to historical documentation strengthens defensibility and reduces audit exposure.
How STEMI Influences Quality, Access, and Equity in Healthcare
STEMI and Quality-Aligned Documentation
From a quality perspective, STEMI documentation supports clarity and continuity, not direct intervention. Accurate STEMI documentation ensures providers maintain a shared understanding of prior high-severity cardiac injury and appropriately factor it into longitudinal care planning.
Quality-aligned documentation reflects that STEMI history informs risk stratification and monitoring decisions rather than ongoing acute management.
STEMI and Care Coordination Across Settings
STEMI often spans multiple care environments, including acute hospitalization, post-acute care, outpatient follow-up, and chronic management. Consistent STEMI documentation across these settings supports safe transitions of care and reduces information loss.
Clear documentation helps the IDT align on cardiac history and future risk considerations.
STEMI and Access to Follow-Up Cardiac Care
STEMI documentation can influence access to appropriate follow-up services by clearly establishing the occurrence of a high-severity cardiac event. Accurate documentation supports timely referral, monitoring, and coordination without unnecessary escalation.
This balance is especially important in longitudinal Medicare care.
Equity Considerations in STEMI Documentation
Access to timely diagnosis and intervention for STEMI is not uniform across populations. Equity-aware documentation may reflect delayed presentation, access barriers, or gaps in follow-up that influence long-term outcomes.
Documenting these contextual factors supports fair interpretation of post-STEMI risk and care needs.
Avoiding Bias in Post-STEMI Risk Assessment
Providers should avoid assumptions about recovery or adherence based solely on demographics or perceived stability. STEMI outcomes and long-term risk are shaped by comorbidities, access, and systemic factors.
Thoughtful documentation supports individualized assessment rather than generalized assumptions.
Frequently Asked Questions about STEMI
1. What is STEMI in healthcare?
STEMI (ST-Elevation Myocardial Infarction) is a subtype of myocardial infarction defined by evidence of acute myocardial injury with ST-segment elevation on an electrocardiogram (ECG). In healthcare documentation, STEMI represents a confirmed, high-severity ischemic cardiac event.
2. Is STEMI considered different from other types of MI?
Yes. STEMI is a specific classification of MI that indicates a particular ECG pattern and is typically associated with more extensive myocardial injury compared to other MI subtypes such as NSTEMI.
3. Does STEMI affect billing or reimbursement directly?
STEMI is not billed independently, but it strongly supports billing and reimbursement by defining the severity and acuity of the cardiac event during the acute episode and informing post-event care decisions.
4. How long should STEMI be documented as an active condition?
STEMI should be documented as an active diagnosis during the acute event and immediate recovery phase. After resolution, it should be transitioned to history of STEMI to reflect its ongoing relevance without implying active ischemia.
5. How does STEMI differ from NSTEMI in documentation?
Both STEMI and NSTEMI are MI subtypes, but STEMI is distinguished by ST-segment elevation on ECG. Documenting the correct subtype improves clarity, risk stratification, and longitudinal record accuracy.
6. What are common STEMI documentation errors?
Common errors include unclear event timing, failure to transition STEMI to historical status, and inconsistent terminology across encounters.
7. Why do reviewers pay attention to STEMI documentation?
Reviewers evaluate whether documentation accurately reflects the severity, timing, and status of cardiac events. STEMI is a high-impact diagnosis that materially influences risk interpretation when documented correctly.
