What is an EMR (Electronic Medical Record)?
An Electronic Medical Record (EMR) is a digital version of a patient’s medical chart that is maintained within a single healthcare organization or practice. EMRs are primarily used to document clinical encounters, diagnoses, medications, treatment plans, and provider notes for care delivered in one setting.
In practice, EMRs function as practice-level documentation systems. They replace paper charts and streamline internal workflows such as charting, ordering, and internal reporting, but they are not inherently designed for broad data exchange across organizations.
While the term EMR is still widely used by providers and healthcare staff, especially in day-to-day operations, it is generally considered more limited in scope than an Electronic Health Record (EHR), which is built for interoperability and longitudinal data sharing.
Key Components of an EMR
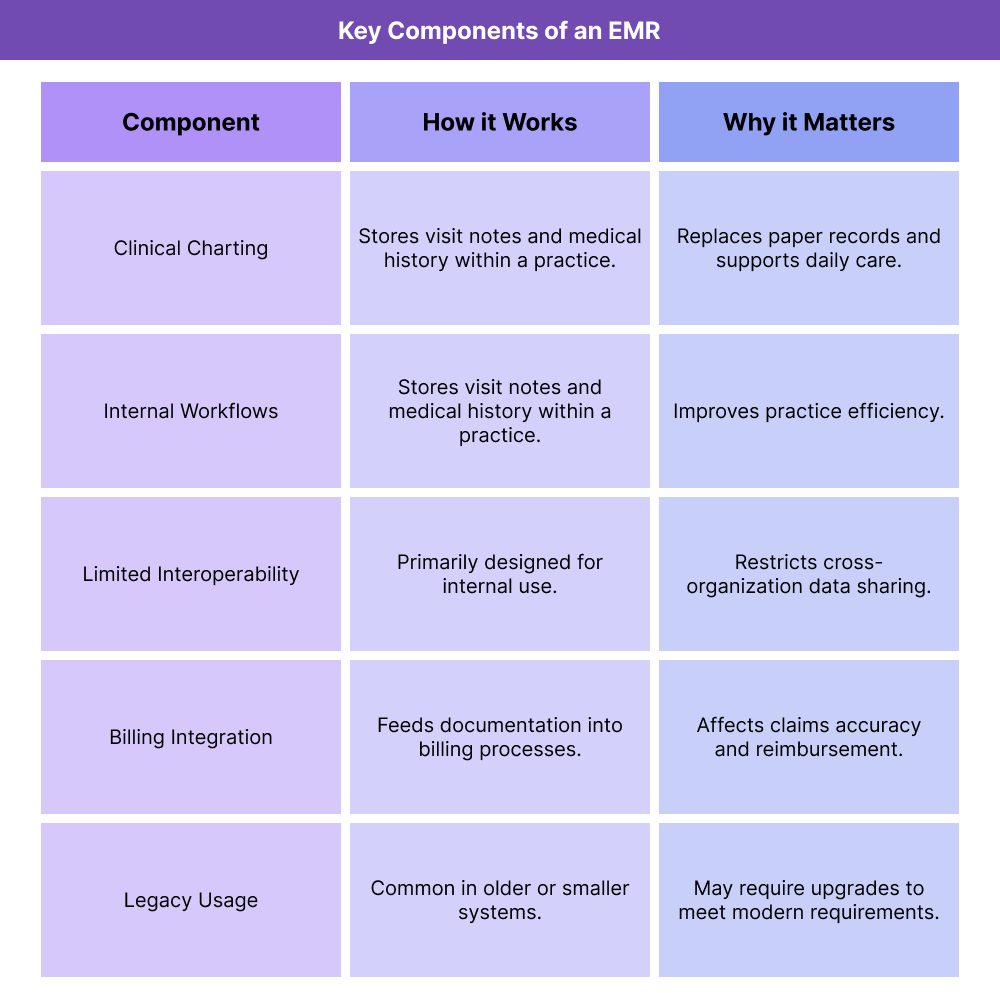
EMRs focus on capturing and organizing clinical information within a single practice or system. These components explain how EMRs are typically used and where their limitations emerge.
Clinical Documentation and Charting
EMRs provide tools for documenting patient visits, including progress notes, diagnoses, medications, allergies, and treatment plans. This documentation supports clinical decision-making and continuity within the practice.
For many providers, the EMR is the primary workspace for daily patient care.
Internal Workflow Support
EMRs are designed to support internal workflows such as scheduling, order entry, and task management. These features help practices operate efficiently without relying on paper-based systems.
However, workflows are usually optimized for internal use rather than coordination with external organizations.
Limited Data Sharing and Interoperability
Unlike EHRs, EMRs are typically not built for seamless data exchange across different healthcare organizations. While some EMRs can export or transmit records, interoperability is often limited or requires additional interfaces.
This limitation becomes more significant as care coordination and reporting requirements increase.
Billing and Administrative Integration
Many EMRs integrate with billing systems to support coding and claims submission. Clinical documentation captured in the EMR feeds administrative workflows such as charge capture and billing.
Accuracy depends on how well documentation aligns with billing requirements, particularly in Medicare-regulated environments.
EMRs in Modern Healthcare Context
Although EMRs remain common, especially in smaller practices or legacy systems, healthcare policy and regulatory frameworks increasingly reference EHRs rather than EMRs. As a result, EMRs may require additional tools or upgrades to meet modern interoperability and reporting expectations.
How EMRs Work in Practice
In practice, EMRs function as practice-centered systems that support documentation and operations within a single organization. They are optimized for internal workflows rather than cross-organizational coordination.
Step 1: Clinical Documentation Within a Single Practice
EMR use begins with clinicians documenting patient encounters, including diagnoses, progress notes, medications, and treatment plans. This documentation supports continuity of care within the practice but is not inherently structured for external sharing.
For many providers, the EMR is the primary workspace for daily clinical activity.
Step 2: Internal Workflow and Order Management
EMRs support internal workflows such as scheduling, order entry, referrals, and task management. These workflows are usually tailored to the needs of a specific practice or specialty.
Because workflows are locally optimized, they may not align cleanly with external billing, reporting, or interoperability requirements.
Step 3: Billing and Coding Integration
Clinical documentation captured in the EMR feeds coding and billing processes, either directly or through integrated practice management systems. Diagnoses and procedures documented in the EMR are used to generate claims.
Misalignment between documentation structure and billing requirements is a common operational challenge, particularly in Medicare billing.
Step 4: Limited Data Exchange Outside the Organization
When patients receive care outside the practice, EMRs often rely on manual processes—fax, scanned documents, or partial exports—to exchange information.
These limitations increase administrative burden and raise the risk of incomplete records during transitions of care.
Step 5: Operational Scaling Constraints
As practices grow or participate in value-based or Medicare programs, EMR limitations become more pronounced. Many organizations eventually need additional systems or migration to EHR platforms to meet expanding requirements.
EMRs in Billing, Reimbursement, and System Limitations
While EMRs can support basic billing workflows, they introduce constraints as reimbursement models and compliance expectations become more complex.
How EMRs Affect Billing and Reimbursement
EMRs support billing by capturing diagnoses, services, and clinical details used for claims submission. However, because EMRs are often optimized for documentation rather than reimbursement logic, gaps can emerge.
Common billing challenges include:
- Incomplete documentation to support medical necessity
- Inconsistent diagnosis capture
- Limited support for complex Medicare billing rules
- Reliance on manual coding review
These issues can lead to denials, delayed payment, or audit risk.
EMRs and Medicare Program Requirements
Many Medicare programs assume EHR-level capabilities, such as structured data capture, reporting, and interoperability. EMRs may struggle to meet these expectations without additional tools.
As a result, organizations using EMRs often layer supplemental systems on top of their core record platform.
System Limitations That Increase Operational Risk
EMR limitations commonly include:
- Minimal interoperability support
- Limited reporting and analytics
- Manual workarounds for quality programs
- Difficulty supporting value-based care models
These constraints increase administrative workload and reduce scalability.
How EMRs Influence Quality, Access, and Equity in Healthcare
EMRs shape care delivery outcomes not just through what they enable, but through what they limit.
EMRs and Quality of Care
EMRs support quality at the practice level by improving documentation consistency and access to patient records. However, lack of interoperability can fragment care when patients receive services from multiple providers.
This fragmentation can reduce visibility into the full clinical picture.
EMRs and Access to Care
EMRs can improve access by streamlining internal workflows and reducing reliance on paper records. At the same time, limitations in data sharing can slow referrals, transitions, and coordination with external providers.
Patients with complex care needs are most affected by these gaps.
Equity Considerations in EMR-Based Care
Equity challenges can arise when EMRs fail to capture social context or exchange data effectively. Patients who receive care across multiple systems—often those facing socioeconomic barriers—may experience fragmented records and duplicative care.
EMR-based practices may need additional processes to ensure continuity and equity in care delivery.
Frequently Asked Questions about EMRs
1. What is an EMR (Electronic Medical Record)?
An EMR is a digital version of a patient’s medical chart used within a single healthcare organization to document and manage clinical care.
2. What is the difference between an EMR and an EHR?
An EMR is typically limited to one practice or system, while an EHR is designed for interoperability and sharing patient data across organizations and care settings.
3. Are EMRs still used in healthcare today?
Yes. Many practices still use EMRs, especially legacy systems, although regulatory frameworks increasingly emphasize EHR capabilities.
4. Can EMRs support Medicare billing?
EMRs can support billing and documentation, but limitations in interoperability and reporting may require additional systems or upgrades to meet Medicare program requirements.
5. Why does CMS and ONC use the term EHR instead of EMR?
CMS and ONC use EHR because it reflects systems designed for data sharing, interoperability, and longitudinal patient records rather than isolated charts.
