What is EF (Ejection Fraction) in Healthcare?
EF (Ejection Fraction) is a clinical measurement that represents the percentage of blood ejected from the heart’s ventricle with each contraction. In healthcare documentation and provider workflows, EF functions less as a numeric value and more as a decision-making input that informs diagnosis, classification, treatment planning, and longitudinal monitoring.
From a provider perspective, EF is most commonly referenced in the context of CHF (Congestive Heart Failure) and related chronic cardiovascular conditions. EF values are used to categorize heart failure subtypes, assess severity, and guide ongoing management decisions across care settings.
Importantly, EF is not a static measurement. It can change over time due to disease progression, treatment response, or acute events. As a result, EF is often revisited throughout a patient’s LOS (Length of Stay) and referenced repeatedly in documentation, care plans, and interdisciplinary discussions.
Because EF directly influences how heart failure is classified and managed, it plays a meaningful role in Chronic Care Management (CCM) workflows. EF trends help justify monitoring frequency, treatment adjustments, and ongoing non–face-to-face clinical oversight in Medicare populations.
In this way, EF operates as a foundational clinical signal—one that contextualizes risk, complexity, and care intensity rather than serving as a standalone diagnostic endpoint.
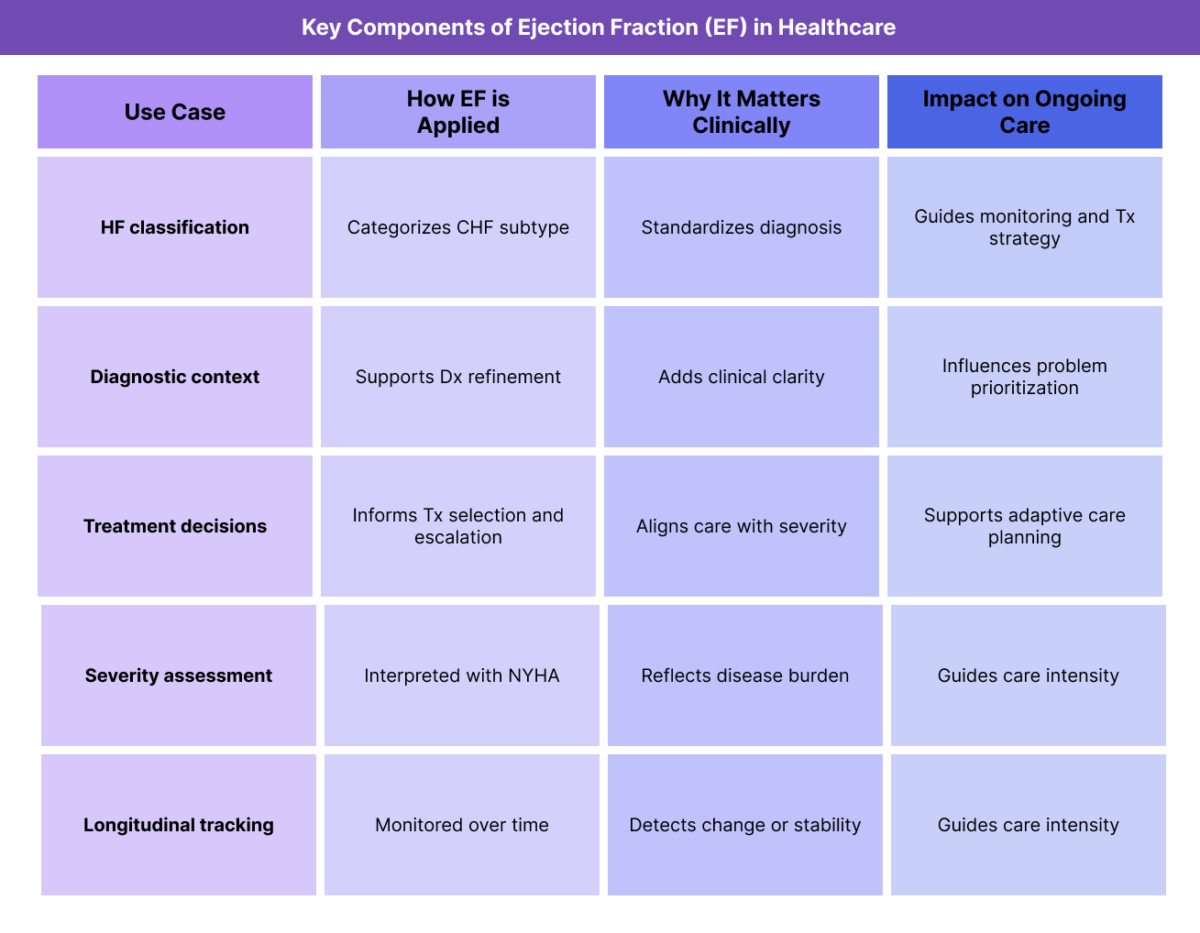
Key Components of how EF Is Used Clinically and Operationally
EF is valuable not because of how it is calculated, but because of how it is used to support clinical reasoning and care delivery.
EF as a Heart Failure Classification Input
EF is commonly used to classify heart failure into subtypes such as HFpEF (Heart Failure with Preserved Ejection Fraction) and HFrEF (Heart Failure with Reduced Ejection Fraction). These classifications affect how providers conceptualize disease trajectory and management strategy.
EF-based classification helps standardize documentation and align care decisions across providers.
EF and Diagnostic Context (Dx)
While EF alone does not establish a diagnosis, it provides important context for Dx (Diagnosis) refinement. EF values help differentiate between heart failure subtypes and may influence how conditions are documented and prioritized on the problem list.
Changes in EF over time may prompt reevaluation of diagnosis or disease severity.
EF and Treatment Planning (Tx)
EF plays a role in guiding Tx (Treatment) decisions, including medication selection, monitoring intensity, and escalation thresholds. Providers often reference EF when determining whether treatment adjustments are warranted or when evaluating response to therapy.
Because EF may improve or decline, it supports adaptive treatment planning rather than fixed interventions.
EF and Functional Severity Assessment
EF is frequently interpreted alongside functional measures such as NYHA Classification. While EF provides a physiologic measurement, NYHA reflects real-world functional impact.
Together, these measures help providers assess overall disease burden and care needs.
EF in Longitudinal Monitoring and CCM
In chronic care contexts, EF is monitored over time to assess disease progression or stability. EF trends may justify continued CCM engagement, adjustments to care plans, or increased coordination.
EF documentation supports the longitudinal narrative required for effective chronic care management.
How EF Is Documented and Used in Practice
EF is referenced repeatedly across the care continuum and must be interpreted in context.
Documenting EF at Start of Care (SOC)
At SOC (Start of Care), EF values are often documented based on prior diagnostic testing or referral information. Providers use this baseline EF to contextualize disease severity and guide initial care planning.
EF documentation at SOC helps frame eligibility and appropriateness for ongoing management.
Using EF During Ongoing Care and LOS
Throughout the patient’s LOS, EF may be revisited when symptoms change, treatment is adjusted, or new diagnostic data becomes available. Providers interpret EF alongside clinical presentation rather than in isolation.
Changes in EF often prompt reassessment of care goals and monitoring strategies.
EF and Interdisciplinary Care Coordination
EF values are commonly referenced by the IDT (Interdisciplinary Team) to align understanding of disease severity and risk. Clear documentation ensures consistent interpretation across disciplines.
Using EF to Support Longitudinal Care Decisions
In chronic and Medicare-focused care models, EF trends support decisions about care continuation, escalation, or transition. EF provides objective context for subjective symptom reports.
EF in Billing, Medical Necessity, and Reimbursement
EF (Ejection Fraction) is not a billable service or standalone determinant of reimbursement, but it plays an important supporting role in how medical necessity, care intensity, and longitudinal services are evaluated—particularly in Medicare-regulated and chronic care contexts.
In provider documentation, EF functions as objective clinical context that helps explain why certain services, monitoring frequency, or care coordination activities are reasonable and necessary for a given patient.
How EF Supports Medical Necessity
Medical necessity is evaluated based on whether services are appropriate given the patient’s condition, risk, and functional impact. EF contributes to this evaluation by helping establish disease severity and complexity, especially in patients with CHF and related cardiovascular conditions.
Documented EF values can help justify:
- increased monitoring frequency
- extended LOS (Length of Stay)
- ongoing care coordination and follow-up
- enrollment in Chronic Care Management (CCM) programs
EF is most effective when it is clearly tied to clinical decision-making rather than listed as an isolated measurement.
EF as Supporting Evidence (Not a Billing Driver)
EF does not independently determine reimbursement. Instead, it supports the broader documentation narrative by reinforcing why:
- treatment plans are structured a certain way
- care is delivered over time rather than episodically
- non–face-to-face management activities are clinically necessary
When EF is referenced appropriately, it strengthens the rationale for billed services without being positioned as the reason for billing itself.
EF and Reimbursement Integrity
Accurate, current EF documentation helps ensure reimbursement reflects true patient complexity. EF values that are outdated, copied forward without context, or inconsistent with documented symptoms can weaken the medical necessity narrative during review.
From a reimbursement integrity standpoint, EF should:
- have a clear source and timeframe
- align with functional status and clinical presentation
- be interpreted in context rather than treated as static
Clear EF documentation reduces the risk of payer questions and supports defensible care delivery.
Medicare Review Considerations Related to EF
During Medicare review, EF may be evaluated as part of the overall clinical picture, particularly when assessing:
- appropriateness of chronic services
- justification for ongoing monitoring or CCM activities
- alignment between documented severity and care intensity
EF documentation that clearly supports care decisions helps reviewers understand why services were delivered and sustained over time.
EF-Related Documentation and Compliance Risks
Because EF (Ejection Fraction) is frequently used to contextualize disease severity and justify longitudinal care, documentation quality matters. Most EF-related compliance issues arise not from incorrect values, but from how EF is referenced and maintained over time.
Common EF-related documentation risks include:
- EF values copied forward without verification
- Missing source or date for EF measurements
- EF documented without interpretation or relevance to care decisions
EF values that conflict with documented symptoms or functional status
Failure to reassess EF relevance as care progresses
When EF is listed passively—without explanation of how it informs Dx, Tx, or monitoring—it can appear disconnected from clinical reasoning during review.
EF and Longitudinal Documentation Expectations
In chronic and Medicare-focused care models, EF should be treated as contextual data, not static background. Providers are not expected to recalculate EF frequently, but they are expected to:
- acknowledge when EF meaningfully informs care decisions
- note when EF data is outdated or externally sourced
- interpret EF alongside current clinical presentation
Clear documentation helps demonstrate that EF is being used intentionally, not reflexively.
System and Workflow Challenges Affecting EF Use
Effective use of EF in care delivery depends heavily on workflow design and data visibility.
Fragmented EF Data Sources
EF values often originate from imaging reports, hospital records, or specialist documentation. When EF data is siloed or difficult to locate, clinicians may rely on outdated information or omit EF context entirely.
Centralized visibility of EF data improves documentation accuracy and care alignment.
Lack of Contextual Prompts
Systems that capture EF as a standalone numeric field without prompting interpretation can encourage shallow documentation. EF is most useful when paired with:
- symptom context
- functional status
- treatment rationale
- Workflow design should support this synthesis.
Inconsistent IDT Awareness
EF is often referenced by multiple disciplines. If EF interpretation is inconsistent across the IDT (Interdisciplinary Team), care planning and coordination may suffer.
Shared understanding reduces misalignment.
EF and Quality, Access, and Equity Considerations
EF influences more than documentation—it affects patient outcomes and fairness in care delivery.
EF and Quality of Care Outcomes
When EF is used appropriately, it supports accurate classification, targeted treatment, and timely reassessment. Tracking EF trends alongside symptoms and function helps providers identify improvement or decline and adjust care accordingly.
Poor EF documentation can obscure risk and delay necessary interventions.
EF and Access to Care
EF values may influence eligibility for services, monitoring intensity, or specialist involvement. Clear documentation supports appropriate access to care and reduces delays caused by incomplete or unclear records.
Equity Considerations in EF Interpretation
Access to diagnostic testing that generates EF measurements is not uniform. Some patients may have outdated EF data due to barriers related to geography, coverage, or care access.
Equity-aware EF use involves:
- acknowledging limitations in available data
- avoiding overreliance on a single measurement
- documenting clinical judgment when EF data is incomplete
This ensures care decisions remain fair and appropriate.
Frequently Asked Questions about EF (Ejection Fraction) in Healthcare
1. What does EF mean in healthcare?
EF stands for Ejection Fraction and refers to the percentage of blood ejected from the heart’s ventricle with each contraction. In healthcare, EF is used as a clinical measurement to assess cardiac function and guide care decisions.
2. Is EF a diagnosis?
No. EF is a measurement, not a diagnosis. It provides context that supports diagnosis and classification of conditions such as heart failure.
3. How does EF support medical necessity?
EF helps establish disease severity and risk, which can justify monitoring frequency, care coordination, and longitudinal services when interpreted alongside clinical findings.
4. Does EF need to be updated frequently?
EF should be revisited when it meaningfully affects care decisions. It does not need constant updating, but outdated EF values should be clearly identified as such.
5. Can EF alone justify Chronic Care Management (CCM)?
EF alone does not justify CCM, but it provides objective context that supports CCM enrollment when combined with chronic conditions such as CHF and documented care needs.
6. What documentation issues commonly involve EF?
Common issues include missing dates, copied-forward values, lack of interpretation, and EF values that do not align with documented symptoms or functional status.
7. How should EF be documented for Medicare review?
EF should be documented with a clear source and timeframe and interpreted in context to explain how it informs care decisions and supports medical necessity.
