What is Dx (Diagnosis) in Healthcare?
Dx (Diagnosis) refers to the identification and clinical determination of a disease, condition, or health problem based on a patient’s signs, symptoms, medical history, and diagnostic findings. A Dx provides the clinical explanation for why a patient requires care and serves as the foundation for treatment decisions, care planning, and documentation throughout an episode of care.
In healthcare operations, Dx is more than a clinical label. It establishes medical necessity, informs the POC (Plan of Care), guides interdisciplinary coordination, and supports billing and compliance requirements—particularly in Medicare-regulated programs. Every major workflow milestone, from SOC (Start of Care) through LOS (Length of Stay) and ultimately DC (Discharge), is influenced by how Dx is defined, documented, and updated.
Dx may evolve over time as additional information becomes available. Initial diagnoses established at intake or SOC are often refined as care progresses, testing is completed, or patient response to treatment is observed. Accurate and timely Dx documentation ensures that care remains aligned with clinical reality and regulatory expectations.
Because Dx underpins care delivery, documentation accuracy is critical. Inconsistent, outdated, or unsupported diagnoses can lead to inappropriate care planning, compliance risk, and reimbursement issues.
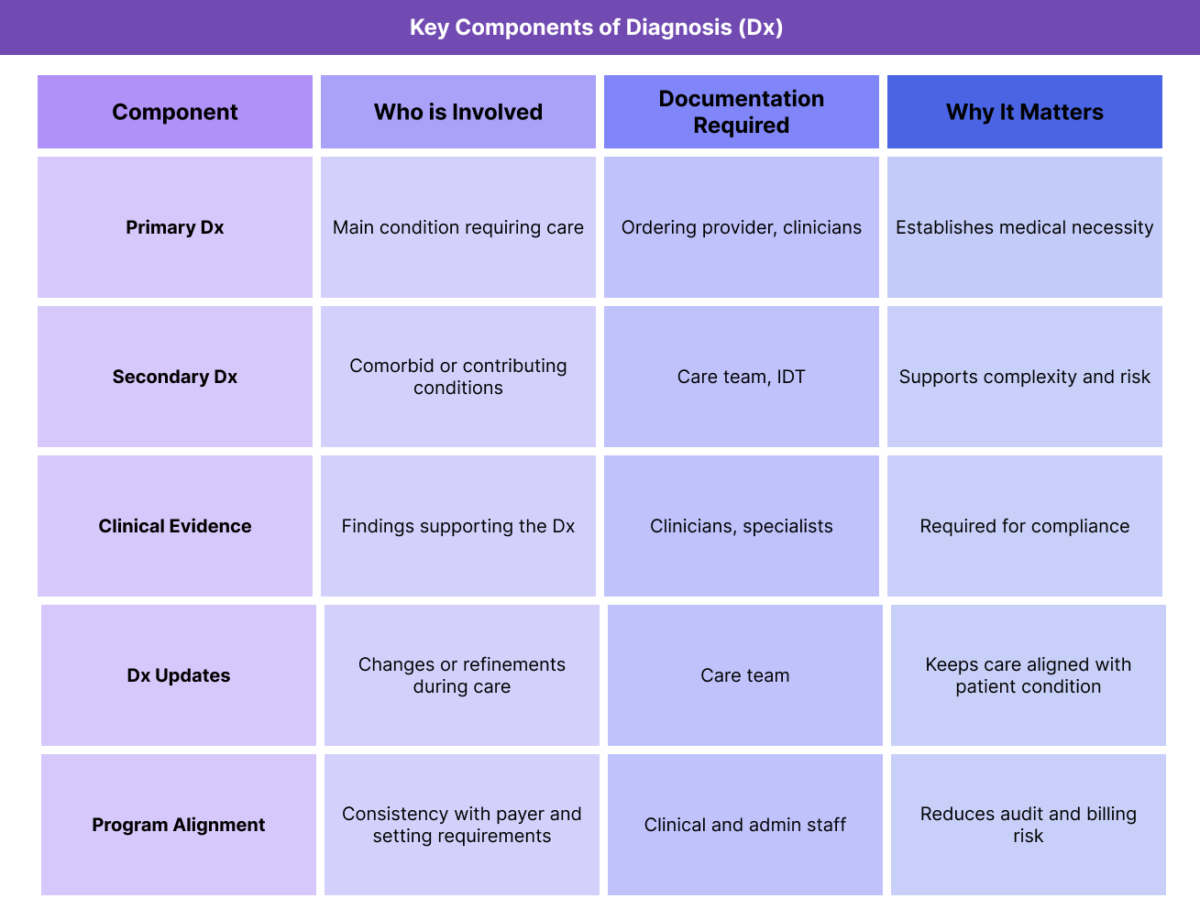
Key Components of Dx (Diagnosis) in Healthcare
Dx is not a single decision made in isolation. It is a structured process shaped by clinical judgment, documentation standards, and care context.
Primary Diagnosis Determination
The primary Dx identifies the main condition responsible for the patient’s need for care. This diagnosis drives the overall focus of treatment, informs the POC, and often anchors billing and reporting.
In Medicare programs, the primary Dx must clearly support medical necessity for the services being delivered.
Secondary and Comorbid Diagnoses
Secondary Dx entries capture additional conditions that affect care complexity, risk, or treatment approach. These may include chronic conditions, functional impairments, or coexisting diseases.
Accurate documentation of secondary Dx supports appropriate care intensity and risk adjustment.
Diagnostic Evidence and Clinical Support
Dx must be supported by clinical evidence such as assessment findings, provider notes, diagnostic tests, or specialist evaluations. Unsupported Dx entries create compliance risk and may be challenged during audits.
Dx Documentation and Updates Over Time
Dx is not static. As patient condition changes, diagnoses may be clarified, added, or resolved. Documentation should reflect these changes consistently across clinical notes and summaries.
Failure to update Dx can result in misaligned care and documentation gaps.
Alignment With Care Setting and Program Rules
Dx requirements vary by care setting and payer. What qualifies as an appropriate Dx in acute care may differ from post-acute or longitudinal Medicare programs. Documentation must align with program-specific expectations.
How Diagnosis (Dx) Works in Practice
Dx plays an active role throughout the lifecycle of a care episode, shaping decisions from intake through discharge.
Establishing Dx at Intake and Start of Care (SOC)
Dx is often first documented during intake or at SOC (Start of Care). At this stage, diagnoses may be provisional, based on referral information, initial assessments, or prior medical records.
These initial Dx entries guide early care planning and service authorization but may require refinement as additional information becomes available.
Using Dx to Inform the Plan of Care (POC)
The POC (Plan of Care) is built around the patient’s Dx. Goals, interventions, visit frequency, and discipline involvement are all selected to address diagnosed conditions.
If Dx documentation is vague or inaccurate, the POC may fail to align with patient needs or regulatory expectations.
Coordinating Dx Across the IDT
Dx informs how the IDT (Interdisciplinary Team) collaborates. Different disciplines may address different aspects of the patient’s diagnoses, requiring shared understanding and consistent documentation.
Misalignment in Dx understanding across the IDT can lead to fragmented care or conflicting documentation.
Monitoring Dx Relevance During LOS
Throughout the patient’s LOS (Length of Stay), clinicians reassess whether the documented Dx continues to reflect the patient’s condition. Changes in symptoms, response to treatment, or new findings may require Dx updates.
Ongoing Dx review helps ensure that continued services remain medically necessary.
Referencing Dx at Discharge (DC)
At DC (Discharge), Dx documentation supports why care concluded. Final notes should reflect whether conditions improved, stabilized, or resolved, and how Dx status aligns with discharge readiness.
Clear Dx documentation at DC supports continuity and compliance.
Dx in Billing, Medical Necessity, and Reimbursement
Diagnosis is one of the primary drivers of how healthcare services are justified, documented, and reimbursed. While Dx itself is not billed, it establishes the clinical rationale that supports nearly all billing activity.
How Dx Establishes Medical Necessity
In Medicare-regulated programs, medical necessity is evaluated based on whether services are reasonable and necessary for the patient’s diagnosed condition. The documented Dx must clearly explain why services are being provided and how they address the patient’s clinical needs.
If the Dx does not logically support the services outlined in the POC (Plan of Care) or the duration of services delivered during the LOS (Length of Stay), claims may be denied or recouped.
Dx and Reimbursement Integrity
Accurate Dx documentation helps ensure that reimbursement aligns with patient complexity and care intensity. Understated or incomplete Dx documentation can result in underpayment, while unsupported Dx entries increase audit risk.
Dx consistency across assessments, progress notes, and summaries is essential to reimbursement integrity.
Dx in Episode-Based and Programmatic Payment Models
In episode-based care models, Dx influences expected resource utilization and care duration. Payers may compare LOS, outcomes, and services delivered against diagnosis-based benchmarks.
Significant deviation without documentation explaining why the Dx warranted extended or intensive care may trigger review.
Dx vs ICD-10 Diagnosis Codes
While closely related, Dx and diagnosis codes are not the same.
Clinical Diagnosis (Dx)
Dx represents the clinician’s determination of the patient’s condition based on assessment and judgment. It is narrative and clinical in nature, describing what is being treated and why.
ICD-10 Diagnosis Codes
ICD-10 codes are standardized alphanumeric representations used for billing, reporting, and data analysis. Codes translate clinical Dx into a structured format required by payers.
Why the Distinction Matters
A clinically accurate Dx that is poorly coded can lead to billing errors, while accurate coding without clinical support creates compliance risk. Alignment between Dx documentation and ICD-10 coding is critical.
Common Dx-Related Compliance and Audit Risks
Dx-related compliance issues often arise from documentation inconsistencies rather than incorrect clinical judgment.
Common risks include:
- Dx not supported by clinical findings
- Outdated Dx that no longer reflects patient condition
- Inconsistent Dx across documentation
- Dx that does not support services delivered
Failure to update Dx during extended LOS
Auditors frequently review Dx alignment with services, documentation, and discharge decisions.
How Dx Influences Quality, Access, and Equity
Diagnosis plays a broader role beyond billing and compliance.
Dx and Quality of Care
Accurate Dx supports targeted care, appropriate interventions, and meaningful outcomes. Misdiagnosis or vague Dx documentation can lead to ineffective or misdirected care.
Dx and Access to Services
Dx influences eligibility for services, program enrollment, and authorization decisions. Incomplete or inaccurate Dx documentation can delay or limit access to needed care.
Equity Considerations in Diagnosis
Implicit bias, language barriers, and access disparities can affect how Dx is established and documented. Equity-aware diagnostic practices seek to ensure Dx accuracy across populations and reduce disparities in care access and outcomes.
Frequently Asked Questions about Diagnosis (Dx) in Healthcare
1. What does Dx mean in healthcare?
Dx is shorthand for Diagnosis and refers to the clinical identification of a disease, condition, or health problem based on a patient’s symptoms, history, and diagnostic findings. Dx explains why care is needed and serves as the foundation for care planning, documentation, and billing justification across healthcare settings.
2. How is diagnosis used in Medicare programs?
In Medicare programs, Dx is used to establish medical necessity for services, guide the POC, and support reimbursement. Medicare reviewers assess whether documented Dx logically supports the services provided during the patient’s LOS and whether Dx documentation is consistent throughout the episode.
3. Can a diagnosis change during an episode of care?
Yes. Dx often evolves as additional information becomes available or as the patient’s condition changes. Diagnoses may be refined, added, or resolved over time. When Dx changes, documentation should be updated to reflect the current clinical picture and justify ongoing services.
4. What is the difference between Dx and ICD-10 codes?
Dx refers to the clinician’s narrative determination of a patient’s condition, while ICD-10 codes are standardized codes used for billing and reporting. Accurate care delivery and compliance require alignment between clinical Dx documentation and ICD-10 coding.
5. Why is accurate diagnosis documentation important for billing?
Billing relies on Dx to demonstrate medical necessity. If Dx documentation does not clearly support the services billed, claims may be denied or audited. Accurate Dx documentation helps ensure reimbursement reflects patient needs and care complexity.
6. How does Dx relate to SOC, LOS, and DC?
Dx is established or confirmed at SOC, guides care delivery throughout LOS, and supports discharge decisions at DC. Together, Dx, SOC, LOS, and DC form the clinical and operational backbone of an episode of care.
7. Can poor Dx documentation affect patient outcomes?
Yes. Inaccurate or vague Dx documentation can lead to misaligned care plans, delayed services, or inappropriate discharge decisions, negatively affecting outcomes and patient experience.
