What is DC (Discharge) in Healthcare?
DC (Discharge) refers to the formal conclusion of a patient’s episode of care within a specific healthcare setting or program. Discharge marks the point at which clinical responsibility transitions away from the current provider or care team, either because care goals have been met, services are no longer medically necessary, or care is being transferred to another setting.
In most care models, DC serves as the official endpoint of care and directly follows the patient’s LOS (Length of Stay). In post-acute and home health settings, DC typically occurs after services initiated at SOC (Start of Care) have been completed and documented according to program requirements.
DC is not merely an administrative event. It is a structured clinical, operational, and compliance-driven process that includes documentation, care transition planning, patient education, and confirmation that discharge criteria have been met. Errors or gaps at discharge can create downstream risks, including readmissions, payment denials, and poor patient experience.
Because DC defines when care formally ends, it plays a critical role in Medicare compliance, quality reporting, and episode closure.
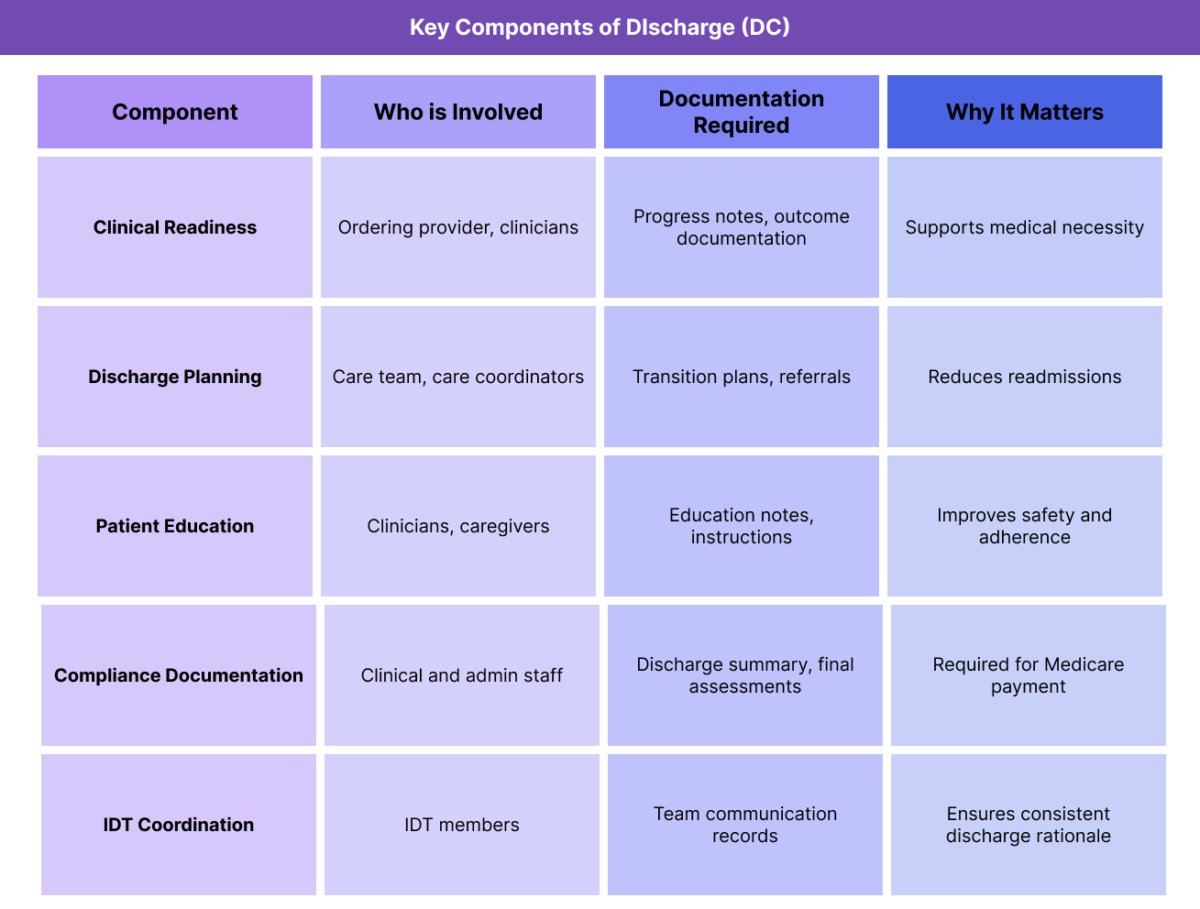
Key Components of DC (Discharge) in Healthcare
Effective discharge requires coordination across clinical, administrative, and regulatory domains. Each component contributes to a safe and compliant transition out of care.
Clinical Readiness for Discharge
Clinical readiness refers to whether the patient has achieved the goals outlined in the POC (Plan of Care) or has reached a point where continued services are no longer medically necessary. This determination must be supported by clinical documentation.
Discharge Planning and Care Transitions
Discharge planning addresses what happens after care ends. This may include follow-up appointments, referrals, medication instructions, or transition to another care setting. Poor discharge planning is a common cause of avoidable readmissions.
Patient and Caregiver Education
Education ensures patients and caregivers understand next steps, warning signs, and ongoing self-management responsibilities. Education gaps can undermine otherwise appropriate discharge decisions.
Documentation and Compliance Requirements
DC documentation must reflect why care ended, how goals were addressed, and whether services were completed as planned. In Medicare-regulated programs, discharge documentation is a frequent audit focus.
Interdisciplinary Coordination at Discharge
Discharge decisions often involve multiple disciplines. Coordination across the IDT (Interdisciplinary Team) helps ensure discharge timing and rationale are consistent and well supported.
How Discharge (DC) Works in Practice
In practice, DC unfolds as a process rather than a single event, with decisions made over time as the patient progresses through care.
Establishing Discharge Criteria Early in the Episode
Effective discharge planning begins early—often at SOC (Start of Care). Establishing clear discharge criteria at the outset helps align expectations across clinicians, patients, and caregivers.
Early clarity reduces the risk of unnecessary LOS extension.
Monitoring Progress Toward Discharge Readiness
Throughout the episode, clinicians assess progress relative to the POC (Plan of Care) and expected LOS (Length of Stay). When patients meet functional or clinical goals, teams begin preparing for discharge.
This ongoing monitoring helps prevent abrupt or poorly coordinated DC decisions.
Coordinating Discharge Across the IDT
Discharge decisions frequently require input from the IDT (Interdisciplinary Team). Nursing, therapy, social work, and care coordination perspectives help ensure discharge is appropriate and safe.
Misalignment within the IDT is a common source of delayed or disputed discharge timing.
Completing Required Discharge Documentation
Before DC can occur, required documentation must be completed. In post-acute and home health settings, this may include final assessments tied to OASIS, discharge summaries, and outcome documentation.
Incomplete documentation at discharge can delay payment or trigger audits.
Transitioning the Patient Out of Care
Once documentation is complete and education is delivered, care formally ends. Responsibility transitions to the patient, caregiver, or next provider, and the episode is closed in the system.
DC in Billing, Reimbursement, and Compliance Oversight
Discharge plays a critical role in determining how and whether care is reimbursed, particularly in Medicare-regulated programs where episode boundaries matter.
How DC Affects Medicare Billing and Payment
DC formally marks the end of a billable episode of care. In post-acute and home health programs, the DC date establishes when services can no longer be billed under the existing episode and when documentation must be finalized to support payment.
Incomplete or inconsistent DC documentation can result in delayed payment, partial reimbursement, or denials. Payers expect the DC rationale to align with clinical documentation recorded throughout the patient’s LOS (Length of Stay) and the goals defined in the POC (Plan of Care).
DC and Episode Closure Requirements
Many Medicare programs impose strict requirements around episode closure at DC. Final assessments, summaries, and certifications must be completed within defined timeframes after discharge.
Failure to meet these requirements can create compliance exposure even when care itself was appropriate.
DC as an Audit and Review Focus Area
Discharge is a frequent audit focal point because it represents a clear, reviewable decision. Auditors often evaluate whether:
- Discharge timing aligns with documented progress
- Medical necessity truly ended at DC
- Required assessments and summaries were completed
- Services did not continue after formal DC
When DC decisions are not clearly justified, organizations may face recoupment or corrective action.
Common Discharge-Related Compliance Risks
Discharge-related issues often stem from operational gaps rather than clinical intent.
Common risks include:
- Premature DC resulting in readmissions
- Prolonged LOS without documented justification
- Missing or late discharge documentation
- Misaligned DC dates across systems
Inadequate patient education at discharge
How DC Influences Quality, Access, and Equity
DC decisions affect more than compliance—they shape patient outcomes and system performance.
DC and Quality of Care Outcomes
Appropriate discharge supports continuity, safety, and goal achievement. Poorly timed DC can lead to adverse events, confusion, or unnecessary return to care.
Quality measurement programs often evaluate outcomes that occur shortly after discharge, making DC decisions especially consequential.
DC and Access to Healthcare Services
Timely and appropriate DC frees capacity for new patients. When discharges are delayed due to administrative or coordination issues, access suffers.
Effective discharge workflows help balance patient needs with system capacity.
Equity Considerations in Discharge Planning
Social determinants such as housing stability, caregiver availability, health literacy, and language access can influence discharge readiness. Equity-aware DC planning accounts for these factors rather than treating them as barriers to throughput.
Failure to address equity considerations can lead to avoidable readmissions or disengagement from follow-up care.
Frequently Asked Questions about Discharge (DC) in Healthcare
1. What does DC mean in healthcare?
DC stands for Discharge and refers to the formal conclusion of a patient’s episode of care. Discharge occurs when clinical goals have been met, services are no longer medically necessary, or care is being transferred to another setting. DC marks the official end of provider responsibility for the episode and triggers final documentation and billing workflows.
2. How is discharge determined in Medicare programs?
In Medicare-regulated programs, discharge decisions must be supported by clinical documentation demonstrating that care goals outlined in the POC have been achieved or that continued services are no longer medically necessary. Discharge timing is reviewed in the context of the patient’s LOS, documented progress, and compliance with required assessments.
3. Is discharge the same as the last visit?
Often, but not always. The last visit may coincide with DC, but discharge is defined by documentation and system status rather than a single encounter. In some cases, documentation or assessments are completed after the final visit to formally close the episode.
4. What documentation is required at discharge?
Discharge documentation typically includes a discharge summary, final assessments, outcome documentation, and evidence of patient education. In settings tied to OASIS, required discharge assessments must also be completed. Missing or late documentation is a common source of compliance risk.
5. Can services be billed after discharge?
No. Services provided after formal DC are generally not billable under the closed episode. Delivering services without re-establishing SOC or opening a new episode can result in denials or recoupment.
6. How does discharge relate to LOS and SOC?
Discharge defines the endpoint of LOS, while SOC defines the beginning. Together, SOC, LOS, and DC form the full lifecycle of an episode of care. Documentation and billing rely on alignment across all three.
7. Why is discharge a focus of audits and reviews?
Discharge is a clear decision point that auditors can easily evaluate. Reviews often focus on whether discharge timing was clinically justified, documentation was complete, and services were appropriately concluded.
