What is CKD (Chronic Kidney Disease) in Healthcare?
CKD (Chronic Kidney Disease) is a long-term condition characterized by progressive impairment of kidney function over time. In healthcare documentation and provider workflows, CKD is treated as a chronic risk and complexity condition, not an episodic diagnosis tied to a single laboratory value.
From an operational standpoint, CKD is especially relevant in adult and Medicare populations because it frequently coexists with cardiovascular disease, including HTN, ASCVD, PAD, CHF, and AFib. Its presence materially increases overall clinical risk and care complexity, even when kidney function decline is mild or stable.
CKD is particularly important in chronic care contexts because progression is often gradual and asymptomatic in early stages. Providers document CKD to explain why ongoing surveillance, care coordination, and reassessment are appropriate despite limited overt symptoms.
Unlike acute kidney injury, CKD is inherently longitudinal. Documentation focuses on severity, progression risk, and interaction with other chronic conditions, supporting sustained care planning across a patient’s LOS (Length of Stay) and transitions of care.
Operationally, CKD often functions as a risk amplifier, helping explain why patients require closer monitoring and more conservative management of comorbid conditions over time.
Key Clinical and Operational Components of CKD in Healthcare
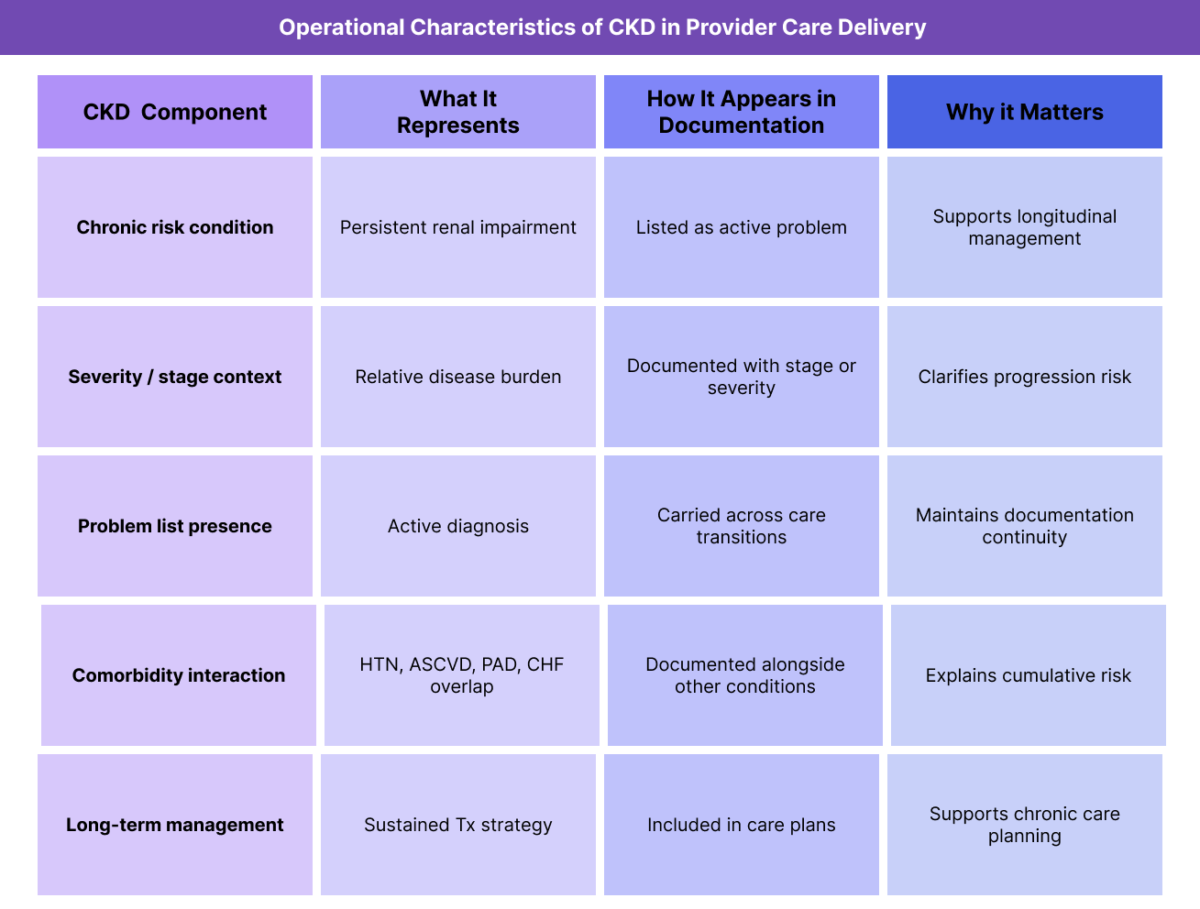
CKD’s importance in care delivery stems from its persistence, staging structure, and interaction with other chronic diseases rather than from isolated diagnostic findings.
CKD as a Chronic Risk Condition
CKD is documented as a chronic condition because impaired kidney function represents ongoing risk for progression, complications, and interaction with other diseases. Even when stable, CKD remains clinically relevant.
This chronic framing supports continued monitoring and reassessment.
CKD Staging and Documentation Context
Providers often document CKD by stage or severity to clarify risk level and progression potential. While staging criteria are clinically defined, the operational value lies in consistent representation of relative disease burden over time.
Clear staging context improves longitudinal documentation clarity.
CKD in Diagnosis and Problem List Management
CKD typically appears on the problem list as an active chronic condition. Maintaining consistent CKD documentation helps ensure continuity across notes, care plans, and transitions of care.
Clear problem list management reduces ambiguity when multiple providers contribute to the record.
CKD and Comorbidity Interaction
CKD frequently interacts with conditions such as HTN, ASCVD, PAD, CHF, and AFib. Providers document CKD to explain how reduced renal function compounds cardiovascular risk and increases overall care complexity.
This interaction supports more comprehensive risk narratives.
CKD and Long-Term Treatment Strategy
CKD management emphasizes long-term Tx (Treatment) and risk mitigation rather than episodic intervention. Providers document CKD to justify sustained management strategies, medication considerations, and monitoring decisions over time.
This reinforces CKD’s role as a chronic care condition.
How CKD Is Managed in Practice
CKD management is documentation-driven and longitudinal, particularly in chronic and Medicare-focused care settings.
CKD at Start of Care (SOC)
At SOC (Start of Care), CKD may be documented based on medical history, referral records, or prior laboratory findings. This establishes CKD as part of the patient’s chronic risk profile and frames baseline management considerations.
Documenting source and context improves clarity.
CKD During Ongoing Care and LOS
Throughout a patient’s LOS, CKD status is referenced to contextualize monitoring decisions, treatment planning, and reassessment needs. Even when stable, CKD remains relevant to care planning.
Consistency across encounters supports longitudinal narratives.
CKD and Interdisciplinary Communication
CKD is a widely recognized chronic condition across disciplines. Clear documentation helps the IDT maintain shared understanding of renal risk and its implications for broader care planning.
This is especially important during transitions of care.
CKD as Context for Care Planning
CKD is often documented to explain why patients require sustained monitoring, conservative management strategies, or coordinated care despite limited symptoms. It provides systemic risk context that complements cardiovascular and metabolic conditions.
CKD in Billing, Reimbursement, and System Limitations
How CKD Supports Medical Necessity Documentation
CKD (Chronic Kidney Disease) is not a billable service, but it provides essential clinical risk context that supports medical necessity for ongoing monitoring, care coordination, and management. In Medicare and other payer environments, CKD documentation helps establish persistent organ dysfunction that justifies longitudinal oversight rather than episodic care.
By documenting CKD as an active condition, providers signal that renal impairment meaningfully affects clinical decision-making even when laboratory values are stable.
CKD and Justification of Longitudinal Care
CKD is frequently used to justify care delivered over time, particularly when progression is slow or asymptomatic. Its chronic nature explains why continued monitoring, reassessment, and conservative management remain appropriate across encounters.
In reimbursement review, CKD often contextualizes:
- duration of care
- frequency of follow-up or monitoring
- medication management decisions
- coordination across specialties
This is especially relevant when CKD coexists with HTN, ASCVD, PAD, CHF, or AFib.
CKD as Supporting Context, Not a Billing Trigger
CKD should not be positioned as the reason a service is billed. Instead, it functions as supporting documentation that helps reviewers understand why care decisions are reasonable given the patient’s renal risk and interaction with other chronic conditions.
CKD adds the most value when integrated into the broader clinical narrative and linked to monitoring or management decisions.
Reimbursement Risk When CKD Is Poorly Documented
CKD documentation can weaken reimbursement support when it is:
- listed without clarity on current relevance or severity
- inconsistently documented across encounters
- copied forward without acknowledgment of stability or progression
- disconnected from care planning or medication considerations
Clear, intentional CKD documentation reduces ambiguity and strengthens defensibility during payer review.
How CKD Influences Quality, Access, and Equity in Healthcare
CKD and Quality-Aligned Care Documentation
From a quality perspective, CKD documentation supports consistency and continuity, not direct intervention. Accurate CKD documentation ensures providers maintain a shared understanding of renal risk and account for it in longitudinal planning.
Quality-aligned documentation reflects that CKD is actively considered in care decisions rather than treated as historical background.
CKD and Care Coordination Across Settings
CKD commonly follows patients across primary care, specialty care, post-acute settings, and home-based services. Consistent documentation helps ensure renal risk is recognized during transitions of care and appropriately factored into ongoing management.
Clear CKD documentation reduces fragmentation when multiple providers contribute to the record.
CKD and Access to Appropriate Services
CKD documentation can influence access to services by clarifying chronic renal risk that may not be evident from acute findings alone. Clear documentation supports appropriate follow-up planning, monitoring frequency, and coordination decisions.
This helps prevent both under-recognition of disease burden and unnecessary escalation.
Equity Considerations in CKD Documentation
CKD prevalence, progression, and management are influenced by social determinants of health, including access to preventive care, diagnostic testing, medications, and specialty services. Equity-aware CKD documentation acknowledges these factors when relevant.
Documenting barriers to consistent monitoring or treatment adherence helps ensure CKD assessment reflects patient reality rather than system access alone.
Avoiding Bias in CKD Interpretation
Providers should avoid assumptions about disease severity or engagement based solely on demographic factors. CKD progression and management are shaped by access, comorbidities, and systemic barriers.
Thoughtful documentation supports fair, individualized assessment of renal disease burden.
Frequently Asked Questions about CKD
1. What is CKD in healthcare?
CKD (Chronic Kidney Disease) is a long-term condition characterized by progressive impairment of kidney function. In healthcare documentation, CKD is used to describe ongoing renal risk and disease burden rather than an acute or isolated laboratory abnormality.
2. Is CKD considered a chronic condition?
Yes. CKD is documented as a chronic condition because reduced kidney function represents persistent risk for progression, complications, and interaction with other chronic diseases over time.
3. Does CKD affect billing or reimbursement directly?
CKD is not billable on its own. However, it supports reimbursement documentation by providing clinical context that explains why longitudinal monitoring, conservative management, and coordinated care are appropriate.
4. How is CKD used in medical necessity review?
CKD supports medical necessity by establishing ongoing organ dysfunction and risk. This helps explain why care continues over time even when laboratory values appear stable.
5. How does CKD interact with cardiovascular conditions?
CKD commonly coexists with HTN, ASCVD, PAD, CHF, and AFib, and can amplify cardiovascular risk. Documenting CKD alongside these conditions helps explain cumulative disease burden.
6. What are common CKD documentation issues?
Common issues include inconsistent problem list use, lack of clarity around severity or relevance, and failure to integrate CKD into longitudinal care planning.
7. Why do reviewers pay attention to CKD documentation?
Reviewers evaluate whether documentation clearly explains chronic risk and supports care decisions. CKD is a widely recognized indicator of complexity and long-term risk when documented consistently.
