What is an EKG or ECG (Electrocardiogram) in Healthcare?
ECG (Electrocardiogram)—also commonly referred to as EKG—is a diagnostic test used to record the electrical activity of the heart. ECG and EKG refer to the same test; both terms appear in healthcare documentation, though ECG is more commonly used in modern clinical records.
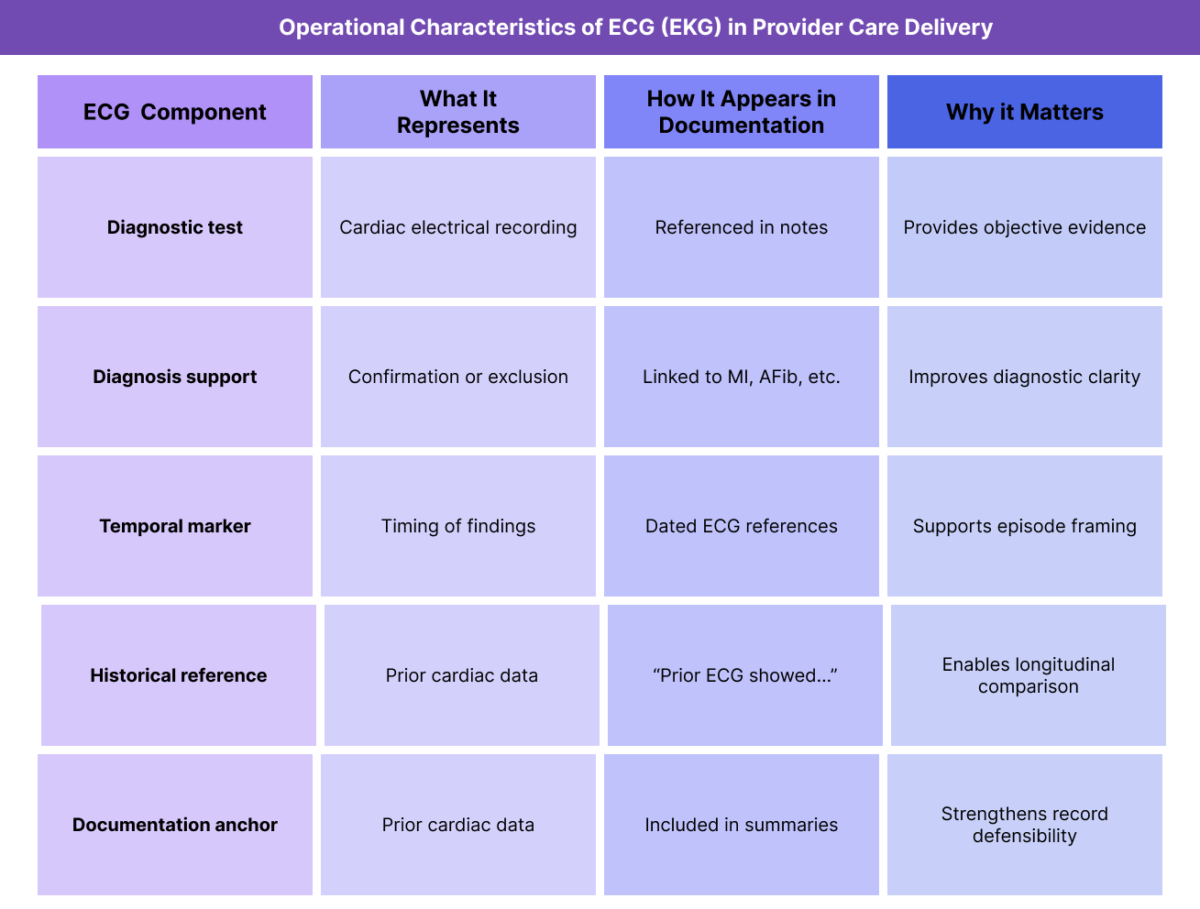
In healthcare documentation and provider workflows, ECG is treated as a diagnostic reference tool, not a diagnosis itself. Providers document ECG findings to support clinical decision-making, confirm or rule out conditions, and provide objective evidence for diagnoses such as MI, STEMI, NSTEMI, AFib, and other cardiac abnormalities.
From an operational standpoint, ECG appears frequently in:
- acute event documentation
- diagnostic summaries
- discharge records
- historical references in longitudinal care
ECG documentation provides objective clinical context that supports diagnoses, episode framing, and longitudinal risk assessment, particularly in adult and Medicare populations.
Key Clinical and Operational Components of ECG in Healthcare
ECG’s importance lies in how it is referenced, documented, and contextualized in the medical record rather than in how it is performed or interpreted.
ECG (EKG) as a Diagnostic Reference
ECG is documented to support or contextualize diagnoses rather than to stand alone. Providers reference ECG findings to confirm rhythm abnormalities, ischemic changes, or prior cardiac injury.
This reference role makes ECG a foundational documentation element in cardiology workflows.
ECG (EKG) in Relation to Cardiac Diagnoses
ECG documentation is commonly linked to diagnoses such as MI, STEMI, NSTEMI, AFib, CAD, and ASCVD. Providers reference ECG findings to establish timing, severity, or classification of cardiac events.
Clear linkage improves diagnostic clarity.
ECG (EKG) and Temporal Context
ECG documentation often includes timing context—such as “on admission,” “during hospitalization,” or “prior ECG showed”—to clarify when findings were recorded relative to symptoms or events.
Temporal clarity is especially important for longitudinal records.
ECG (EKG) in Diagnosis and Problem List Context
ECG results themselves do not appear on the problem list, but they frequently support problem list diagnoses. Providers reference ECG findings to justify adding, updating, or resolving cardiac diagnoses.
This supporting role strengthens documentation integrity.
ECG (EKG) and Longitudinal Care Planning
Historical ECG references help providers understand prior cardiac findings and changes over time. This supports monitoring decisions and continuity of care, especially for patients with chronic cardiovascular disease.
How ECG (EKG) Is Documented and Used in Practice
ECG documentation varies depending on whether it supports an acute event or provides historical context.
ECG (EKG) During Acute Cardiac Evaluation
During acute evaluation, ECG is documented to support diagnosis classification and event timing. Providers reference ECG findings to confirm or exclude conditions such as STEMI or NSTEMI.
Documentation focuses on existence and relevance, not waveform interpretation.
ECG (EKG) in Longitudinal and Historical Records
In longitudinal care, ECG is referenced historically to provide context for prior cardiac findings. Providers may note prior ECG abnormalities or stability to support ongoing risk assessment.
Historical references support continuity across encounters.
ECG (EKG) and Interdisciplinary Communication
Clear ECG documentation helps the IDT understand diagnostic context without requiring interpretation detail. This shared understanding supports coordinated care and consistent decision-making.
ECG (EKG) in Transitions of Care
ECG findings are often summarized during transitions of care to provide receiving providers with objective cardiac context. Accurate references reduce ambiguity and prevent duplication.
ECG or EKG in Billing, Reimbursement, and System Limitations
How ECG (EKG) Supports Medical Necessity Documentation
ECG (Electrocardiogram / EKG) is not a billable diagnosis, but it is a high-value diagnostic service whose documentation plays a critical role in supporting medical necessity. In Medicare and other payer environments, ECG documentation provides objective clinical evidence that justifies diagnostic decision-making, episode framing, and downstream care.
Accurate ECG documentation helps demonstrate that cardiac evaluation was clinically appropriate based on presenting risk, symptoms, or known cardiovascular history.
ECG (EKG) as Objective Evidence in Cardiac Evaluation
From a reimbursement perspective, ECG functions as objective diagnostic support rather than a standalone justification. Providers reference ECG findings to explain why specific diagnoses were made, ruled out, or monitored over time.
ECG documentation commonly supports:
- classification of MI subtypes (e.g., STEMI vs NSTEMI)
- confirmation of rhythm abnormalities (e.g., AFib)
- evaluation of ischemic risk in CAD or ASCVD
This linkage strengthens the clinical narrative during review.
ECG (EKG) and Episode Framing
ECG timing is often used to frame cardiac episodes. Documentation may reference ECGs obtained at presentation, during hospitalization, or as part of follow-up evaluation to clarify when diagnostic findings occurred relative to symptoms or events.
Clear temporal context reduces ambiguity during reimbursement review.
Reimbursement Risk When ECG (EKG) Is Poorly Documented
ECG documentation can weaken reimbursement support when:
- ECGs are referenced without timing or context
- diagnostic relevance is unclear
- findings are disconnected from documented diagnoses
- historical ECGs are misrepresented as current
Clear, contextual ECG documentation improves defensibility and reduces audit exposure.
How ECG Influences Quality, Access, and Equity in Healthcare
ECG (EKG) and Quality-Aligned Documentation
From a quality perspective, ECG documentation supports clarity and continuity, not interpretation. Accurate ECG documentation ensures providers share a common understanding of objective cardiac findings and incorporate them appropriately into care planning.
Quality-aligned documentation reflects ECG’s role as supporting evidence rather than a clinical conclusion.
ECG (EKG) and Care Coordination Across Settings
ECG findings frequently move with patients across care settings, including inpatient, outpatient, post-acute, and longitudinal care. Consistent documentation helps receiving providers understand prior cardiac evaluations without repeating testing unnecessarily.
Clear ECG references support smoother transitions of care.
ECG (EKG) and Access to Diagnostic Evaluation
ECG documentation can influence access to additional evaluation by clarifying whether cardiac assessment has already occurred and what findings were present. This supports appropriate escalation—or de-escalation—of care.
Accurate documentation helps balance access with clinical appropriateness.
Equity Considerations in ECG (EKG) Documentation
Access to timely ECG evaluation is not uniform across populations. Equity-aware documentation may note delays, limitations in testing availability, or gaps in follow-up that affect interpretation of cardiac risk.
Documenting these factors supports fair assessment of care quality and outcomes.
Avoiding Bias in ECG (EKG) Interpretation Context
Providers should avoid assumptions based on incomplete ECG history or access gaps. ECG findings should be contextualized within the patient’s overall clinical picture rather than treated as definitive in isolation.
Thoughtful documentation supports individualized, equitable care assessment.
Frequently Asked Questions about ECG
1. What is ECG or EKG in healthcare?
ECG (Electrocardiogram), also called EKG, is a diagnostic test that records the electrical activity of the heart. In healthcare documentation, ECG provides objective evidence that supports cardiac diagnoses and clinical decision-making.
2. Are ECG and EKG the same thing?
Yes. ECG and EKG refer to the same diagnostic test. Both terms appear in medical records, though ECG is more commonly used in modern documentation.
3. Does ECG (EKG) affect billing or reimbursement directly?
ECG itself is a billable diagnostic service, but its documentation also supports reimbursement by providing objective evidence that explains diagnostic and care decisions.
4. How is ECG (EKG) used in medical necessity review?
ECG supports medical necessity by demonstrating that cardiac evaluation was clinically appropriate. Reviewers look for clear linkage between ECG findings and documented diagnoses or care decisions.
5. How does ECG (EKG) relate to MI, STEMI, and NSTEMI?
ECG findings are used to help classify myocardial infarctions. For example, ST-segment elevation on ECG supports STEMI classification, while absence of ST elevation supports NSTEMI classification.
6. What are common ECG (EKG) documentation issues?
Common issues include missing timing context, unclear relevance to diagnoses, and inconsistent references to historical versus current ECG findings.
7. Why do reviewers pay attention to ECG (EKG) documentation?
Reviewers evaluate whether ECG documentation clearly supports diagnoses and care decisions. ECG is a foundational diagnostic tool whose documentation strengthens clinical narratives when used correctly.
