What is NYHA (New York Heart Association) Classification in Healthcare?
NYHA (New York Heart Association) Classification is a standardized functional classification system used to describe the severity of heart failure based on a patient’s physical activity tolerance and symptom burden. Rather than focusing on anatomy or test results, NYHA classification reflects how a cardiovascular condition affects a patient’s day-to-day functioning.
In provider workflows, NYHA functions as a functional severity shorthand. It allows clinicians to communicate how limited a patient is in real-world terms, using a consistent and widely recognized framework. NYHA is most commonly used in the context of CHF (Congestive Heart Failure), but its relevance extends to longitudinal care planning, monitoring, and documentation across settings.
Unlike measurements such as EF (Ejection Fraction), which describe cardiac function physiologically, NYHA classification captures functional impact. This makes it especially valuable in chronic and Medicare-focused care, where functional status often determines care intensity, monitoring needs, and service eligibility.
NYHA classification is not static. Patients may move between NYHA classes over time as symptoms worsen or improve. Because of this variability, NYHA is frequently reassessed throughout a patient’s LOS (Length of Stay) and referenced in longitudinal documentation.
From an operational standpoint, NYHA helps providers translate clinical findings into actionable care decisions, making it a key input for chronic care management, interdisciplinary coordination, and discharge planning.
Key Components of NYHA Functional Classification
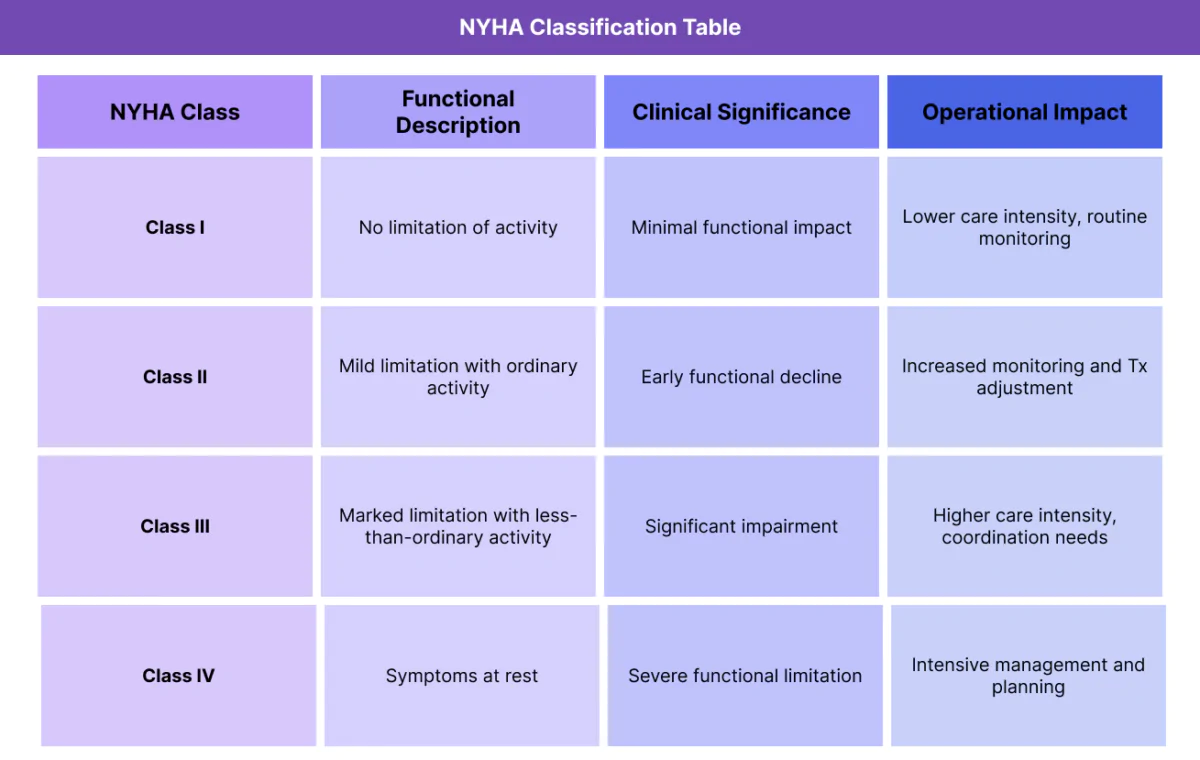
NYHA classification is organized into four functional classes that describe increasing levels of limitation. These classes are defined by symptom presence during activity, not by diagnostic test results.
NYHA Class I — No Limitation of Physical Activity
Patients in NYHA Class I have heart disease but do not experience symptoms with ordinary physical activity. Daily activities can be performed without undue fatigue, dyspnea, or discomfort.
Operationally, NYHA Class I often indicates lower immediate care intensity, though ongoing monitoring may still be required in chronic conditions.
NYHA Class II — Mild Limitation of Physical Activity
NYHA Class II patients are comfortable at rest but experience symptoms with ordinary physical activity. These limitations may affect endurance or tolerance for sustained activity.
Class II often represents an early signal of functional decline and may prompt closer monitoring or adjustments to Tx (Treatment).
NYHA Class III — Marked Limitation of Physical Activity
Patients classified as NYHA Class III experience symptoms with less-than-ordinary activity and are comfortable only at rest. Functional impairment is significant and often affects independence.
NYHA Class III frequently correlates with ADL and IADL challenges and increased care coordination needs.
NYHA Class IV — Inability to Carry Out Physical Activity Without Symptoms
NYHA Class IV patients experience symptoms at rest and are unable to perform any physical activity without discomfort. This represents severe functional impairment and high clinical risk.
Class IV often drives intensive monitoring, interdisciplinary involvement, and careful discharge planning.
NYHA as a Functional, Not Diagnostic, Framework
Importantly, NYHA classification does not diagnose heart failure or specify etiology. Instead, it categorizes functional impact, making it complementary to diagnostic terms such as CHF and classification systems like HFpEF and HFrEF.
How NYHA Is Used in Practice
NYHA classification is applied throughout the care continuum to support consistent communication and decision-making.
Using NYHA at Start of Care (SOC)
At SOC, NYHA classification helps establish a functional baseline that complements diagnostic findings. Providers document NYHA class to contextualize disease severity and inform initial care planning.
This baseline is often used alongside EF and CHF diagnosis to guide monitoring expectations.
NYHA in Ongoing Monitoring and LOS
Throughout a patient’s LOS, NYHA class may be reassessed as symptoms change or treatment is adjusted. Movement between NYHA classes provides a functional signal of improvement or decline.
Documenting these changes supports longitudinal care narratives.
NYHA and Treatment Planning
NYHA classification often influences Tx decisions by indicating how aggressively symptoms should be managed and how closely patients should be monitored. Higher NYHA classes generally correlate with increased care intensity.
NYHA and Chronic Care Contexts
Because NYHA reflects functional limitation rather than anatomy, it aligns closely with Chronic Care Management (CCM) goals. NYHA helps justify ongoing oversight, care coordination, and non–face-to-face management in patients with chronic cardiovascular disease.
NYHA in Billing, Medical Necessity, and Reimbursement
NYHA as Functional Support for Medical Necessity
NYHA classification supports medical necessity by documenting the functional impact of cardiovascular disease rather than relying solely on diagnoses or test results. In Medicare-regulated care, functional limitation is often central to determining whether services are reasonable and necessary.
By describing how symptoms limit ordinary activity, NYHA helps explain why monitoring, follow-up, or coordinated care is clinically appropriate over time.
NYHA and Justification of Care Intensity
NYHA class can help contextualize why a patient requires a higher level of care intensity compared to another patient with the same diagnosis. For example, a patient with CHF documented as NYHA Class III presents a different care burden than one documented as Class I, even if both share the same underlying condition.
This functional distinction supports documentation that aligns care delivery with patient need.
NYHA in Longitudinal Reimbursement Review
During retrospective review, payers often assess whether care delivered over time aligns with documented severity. NYHA classification helps reviewers understand how functional limitation persists or evolves across a patient’s LOS, supporting the duration and scope of services provided.
Consistent NYHA documentation across encounters strengthens the longitudinal reimbursement narrative.
NYHA as Context, Not a Billing Trigger
NYHA should never be positioned as the reason a service is billed. Instead, it serves as supporting clinical context that explains why billed services make sense given the patient’s functional status.
NYHA adds the most value when it is clearly tied to care planning, monitoring decisions, or reassessment—not when it is listed in isolation.
Reimbursement Risk When NYHA Is Poorly Documented
NYHA documentation that lacks functional explanation, is copied forward without reassessment, or conflicts with symptom documentation can weaken reimbursement support. Reviewers may question whether functional severity was actively considered when planning care.
Clear, contextual NYHA documentation reduces ambiguity and supports defensible billing.
NYHA and Quality, Access, and Equity Considerations
NYHA and Quality of Care Alignment
NYHA classification supports quality care by helping providers align interventions with functional severity. When NYHA is reassessed appropriately, it can signal improvement or decline earlier than diagnostic data alone, allowing for timely treatment adjustments.
Tracking NYHA over time helps demonstrate responsive, patient-centered care.
NYHA and Care Coordination Across Settings
Because NYHA is widely recognized, it improves communication across care teams and settings. A clearly documented NYHA class allows different providers to quickly understand functional limitations and adjust care expectations accordingly.
This consistency supports smoother transitions and better continuity of care.
NYHA and Access to Services
Functional classification often influences access to services such as follow-up frequency, care coordination, or supportive interventions. NYHA documentation can help ensure patients with significant limitations receive appropriate attention, even when diagnostic findings alone do not fully capture severity.
Clear NYHA use supports equitable access to necessary services.
Equity Considerations in NYHA Assessment
NYHA relies on patient-reported activity tolerance, which introduces equity considerations. Language barriers, health literacy, cultural norms, and socioeconomic context can all influence how patients describe symptoms and limitations.
Equity-aware NYHA documentation involves clarifying what “ordinary activity” means for the individual patient and documenting context when symptom reporting may be incomplete or ambiguous.
Avoiding Bias in Functional Classification
Providers should avoid assumptions about functional capacity based on age, appearance, or diagnosis alone. NYHA classification should reflect the patient’s actual lived experience, supported by clear documentation.
Thoughtful NYHA use helps reduce bias and promotes fair, individualized care decisions.
Frequently Asked Questions about NYHA Classification in Healthcare
1. What is NYHA classification in healthcare?
NYHA (New York Heart Association) classification is a standardized functional classification system used to describe the severity of heart failure based on how symptoms limit a patient’s physical activity. In healthcare documentation, NYHA provides a consistent way to translate subjective symptom burden into an objective, widely recognized severity category.
NYHA is not a diagnosis or a treatment. It functions as a clinical and documentation standard that helps providers, care teams, and reviewers understand how cardiovascular disease affects a patient’s day-to-day functioning.
2. Is NYHA a compliance or clinical standard?
NYHA is a clinical classification standard, not a regulatory requirement. However, because it is widely recognized and consistently applied across cardiology and chronic care settings, it often functions as a de facto documentation standard.
When used appropriately, NYHA supports compliance by improving clarity, consistency, and defensibility in records reviewed by payers or auditors.
3. Does NYHA need to be reassessed regularly?
NYHA does not require scheduled or routine reassessment. It should be updated only when there is a meaningful change in functional status that affects how the patient’s condition is described.
NYHA is reassessed because the patient changes—not because of a documentation cadence or compliance rule.
4. Does NYHA classification affect billing or reimbursement?
NYHA is not billable and does not directly affect reimbursement. However, it can support billing review by providing functional context that explains why the level, duration, or intensity of care was appropriate for the patient.
When NYHA aligns with symptoms, activity tolerance, and care decisions, it strengthens the overall documentation narrative during review.
5. How is NYHA different from EF (Ejection Fraction)?
EF is a physiologic measurement of cardiac function, while NYHA is a functional classification describing how symptoms affect daily activity. EF explains what the heart is doing; NYHA explains how the patient is functioning.
They are complementary and often documented together, but they serve different purposes.
6. What are common documentation problems with NYHA classification?
Common issues include documenting a NYHA class without functional support, copying NYHA forward across encounters despite symptom changes, or listing a class that conflicts with documented activity tolerance or ADL/IADL status.
These patterns can make documentation appear templated rather than clinically grounded.
7. Why do auditors or reviewers pay attention to NYHA?
Reviewers do not look for NYHA specifically, but they do evaluate whether documentation clearly explains functional severity. NYHA is one of the most recognizable frameworks for doing so in heart failure documentation.
When NYHA is present and consistent, it can reduce ambiguity during review.
8. Does NYHA classification influence care quality?
Defensible NYHA documentation aligns with symptom descriptions, includes brief functional context, is updated only when clinically appropriate, and remains consistent across provider and interdisciplinary notes.
This treats NYHA as a functional classification standard, not a checkbox.
