What is an EHR (Electronic Health Record)?
An Electronic Health Record (EHR) is a digital system designed to create, store, and share a patient’s health information across multiple providers and care settings. Unlike records confined to a single practice, EHRs are built to support longitudinal patient records, interoperability, and standardized reporting.
In practice, an EHR aggregates clinical data such as diagnoses, medications, lab results, care plans, and encounter history, while also supporting workflows tied to billing, quality programs, and regulatory compliance. EHRs are the primary technology platform referenced in Medicare, CMS, and ONC policy frameworks.
From an operational perspective, EHRs sit at the intersection of clinical care, reimbursement, and oversight. How an EHR captures, structures, and exchanges data directly affects everything from claims submission and quality reporting to audit readiness and care coordination.
Key Components of an EHR
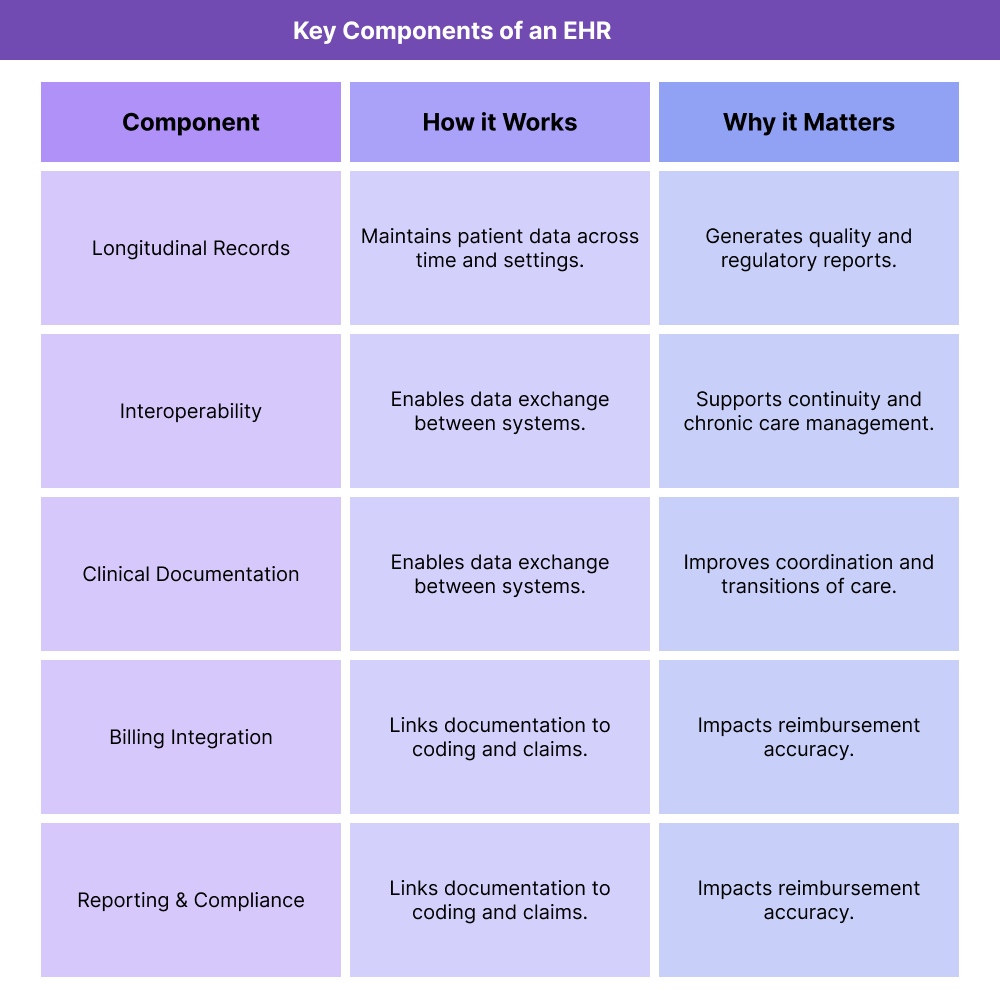
EHRs are complex systems that support far more than digital charting. These core components explain how EHRs function and why they are central to modern healthcare operations.
Longitudinal Patient Health Records
EHRs are designed to maintain a comprehensive, longitudinal view of a patient’s health over time. This includes information from multiple encounters, providers, and care settings.
This longitudinal structure supports continuity of care and reduces fragmentation, particularly for patients with chronic or complex conditions.
Interoperability and Data Exchange
A defining feature of EHRs is their ability to share data across organizations. Interoperability enables information exchange between hospitals, clinics, post-acute providers, labs, and other stakeholders.
In Medicare contexts, interoperability supports care coordination, transitions of care, and reporting requirements tied to quality and value-based programs.
Clinical Documentation and Workflow Support
EHRs provide structured tools for clinical documentation, including progress notes, orders, medication management, and care plans. These tools are designed to standardize documentation while supporting clinical decision-making.
Documentation captured in the EHR feeds downstream workflows such as billing, quality measurement, and compliance review.
Billing, Coding, and Administrative Integration
Most EHRs integrate with billing and coding workflows, either directly or through connected systems. This integration helps align clinical documentation with claims submission and reimbursement requirements.
In Medicare-regulated environments, EHR configuration can significantly affect denial rates, audit risk, and operational efficiency.
Reporting, Quality Measurement, and Compliance Support
EHRs support reporting for quality programs, performance measurement, and regulatory compliance. Structured data captured in the EHR is used to generate reports required by payers and oversight entities.
Accurate reporting depends on consistent documentation and correct system configuration.
How EHRs Work in Practice
In practice, Electronic Health Records function as the operational backbone of healthcare delivery, documentation, and reporting. EHRs connect clinical workflows with administrative, billing, and compliance processes across settings and over time.
Rather than being used only at the point of care, EHRs support a continuous lifecycle of data capture, exchange, and reuse.
Step 1: Clinical Documentation at the Point of Care
EHR use begins with clinicians documenting patient encounters, diagnoses, medications, orders, and care plans. This documentation forms the primary clinical record and is structured to support downstream use.
In Medicare-regulated environments, how data is entered into the EHR directly affects billing accuracy, quality reporting, and audit defensibility.
Step 2: Data Sharing and Interoperability Across Settings
EHRs enable information to be shared between providers, facilities, and care settings. This is especially important for patients who move between inpatient, outpatient, and post-acute care.
Interoperability supports transitions of care, reduces duplication, and improves continuity—key priorities in Medicare and value-based care programs.
Step 3: Billing, Coding, and Claims Support
Clinical documentation captured in the EHR feeds coding and billing workflows. Diagnoses, procedures, and care details must be structured correctly to support claims submission.
Misalignment between documentation and billing logic is a common cause of denials, audits, and reimbursement delays.
Step 4: Quality Measurement and Reporting
EHR data is used to calculate quality measures, monitor performance, and generate required reports. Many Medicare quality programs rely on structured EHR data rather than manual abstraction.
Incomplete or inconsistent documentation can negatively affect reported outcomes and performance metrics.
Step 5: Compliance, Audits, and Oversight
EHRs play a central role in compliance and audit workflows. Auditors often rely on EHR records to assess medical necessity, documentation completeness, and consistency across encounters.
Strong EHR configuration and disciplined documentation practices improve audit readiness and reduce compliance risk.
EHRs in Billing, Reimbursement, and System Limitations
EHRs significantly influence how healthcare organizations bill for services and comply with payer requirements.
How EHRs Affect Billing and Reimbursement
EHRs support billing by linking clinical documentation to coding and claims generation. Accurate data capture helps ensure services are billed correctly and paid appropriately.
However, EHR limitations—such as poorly designed templates or inconsistent workflows—can lead to coding errors and reimbursement issues.
EHR Configuration and Denial Risk
System configuration matters. Default settings, templates, and required fields influence what data is captured and how it is used.
Common risks include:
- Missing or inconsistent diagnoses
- Incomplete documentation to support medical necessity
- Data that does not align with billing or quality logic
- System Limitations and Operational Challenges
Despite their central role, EHRs can introduce challenges, including:
- Documentation burden for clinicians
- Fragmented workflows across modules
- Interoperability gaps between systems
- Reporting complexity for quality programs
Organizations often need additional processes or tools to fully operationalize EHR data.
How EHRs Influence Quality, Access, and Equity in Healthcare
Beyond operations, EHRs shape how care is delivered and evaluated.
EHRs and Quality of Care
When used effectively, EHRs support better care coordination, decision-making, and monitoring of patient outcomes. Structured data enables proactive management of chronic conditions and preventive care.
EHRs and Access to Care
EHRs can improve access by enabling telehealth, remote documentation, and coordination across providers. At the same time, usability challenges or poor workflow design can slow care delivery.
Equity Considerations in EHR Use
EHR design and data practices can influence equity. Missing social context, inconsistent data capture, or limited interoperability can obscure disparities and barriers to care.
Equity-aware EHR use emphasizes accurate data capture, inclusive documentation, and interoperability across care settings.
Frequently Asked Questions about EHRs
1. What is an EHR (Electronic Health Record)?
An EHR is a digital system designed to create and share a patient’s health information across providers and care settings, supporting longitudinal records, billing, quality reporting, and compliance.
2. What is the difference between an EHR and an EMR?
An EHR is designed for interoperability and data sharing across organizations, while an EMR is typically limited to documentation within a single practice or system. (The EMR page will go deeper on this distinction.)
3. Why are EHRs important in Medicare programs?
EHRs support documentation, billing, quality reporting, and compliance requirements defined by CMS and Medicare programs.
4. How do EHRs affect billing and reimbursement?
EHR documentation feeds coding and claims workflows. Inaccurate or incomplete data can lead to denials, audits, or delayed payment.
5. Do EHRs improve care coordination?
Yes. EHR interoperability supports data exchange across settings, improving transitions of care and continuity for complex patients.
6. Are EHRs required by Medicare?
While Medicare does not mandate a specific vendor, many Medicare programs and reporting requirements assume the use of certified EHR technology.
7. Can EHR limitations create compliance risk?
Yes. Poor configuration, inconsistent documentation, or incomplete data capture can increase audit and compliance exposure.
