What is PDGM (Patient Driven Groupings Model) in Home Health?
The Patient-Driven Groupings Model (PDGM) is Medicare’s payment methodology for home health services that determines reimbursement based on patient characteristics rather than therapy volume. PDGM applies to Medicare home health episodes and is designed to align payment more closely with patient needs, clinical complexity, and timing of care.
Under PDGM, Medicare reimbursement is driven by factors such as the patient’s clinical condition, functional status, admission source, timing of the episode, and the presence of comorbidities. These factors are captured through clinical documentation and standardized assessments rather than the number of therapy visits delivered.
Operationally, PDGM fundamentally changed how Home Health Agencies (HHAs) approach documentation, intake, and care planning. Accurate clinical assessment and documentation are now central to both payment and compliance, making PDGM tightly linked to OASIS data, coding practices, and audit readiness.
Key Components of PDGM
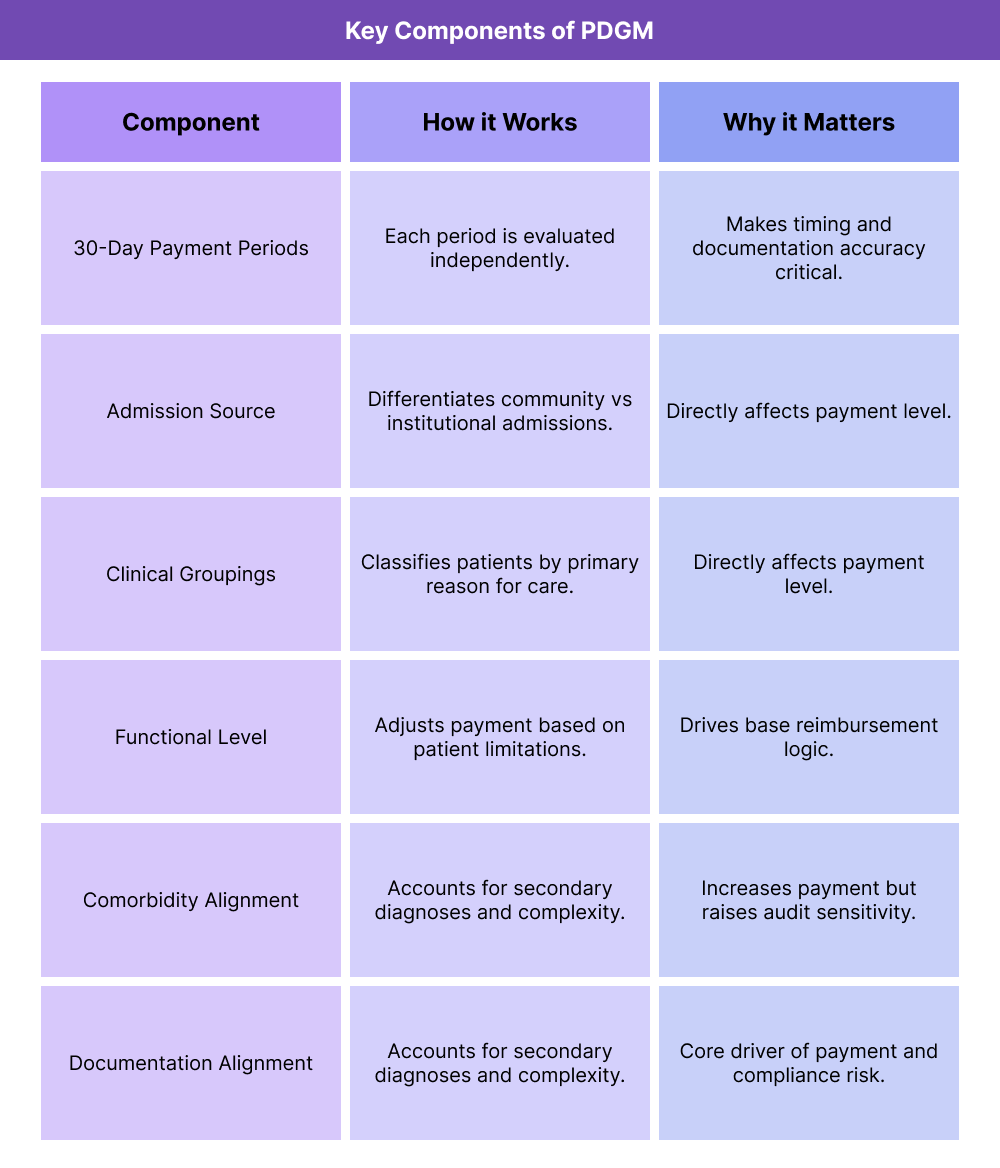
PDGM is built around a structured grouping methodology that classifies patients into payment groups based on defined characteristics. Understanding these components is essential for HHAs, billing teams, and compliance leaders.
PDGM Episode Structure and Timing
Under PDGM, home health payment is based on defined 30-day payment periods rather than longer episode structures used previously. Each payment period is evaluated independently based on patient characteristics and documentation during that timeframe.
Timing matters operationally because changes in patient status, documentation gaps, or delayed assessments can directly affect reimbursement for each period.
Admission Source Classification in PDGM
PDGM distinguishes between community admissions and institutional admissions. Admission source classification affects payment because patients transitioning from hospitals, IRFs, or SNFs are assumed to have higher acuity and resource needs.
Accurate documentation of admission source is critical, as misclassification can lead to incorrect payment and compliance risk.
Clinical Groupings Under PDGM
Patients are assigned to clinical groupings based on the primary reason for home health services. These groupings reflect the type of care being delivered, such as post-surgical care, neurological rehabilitation, or chronic condition management.
The clinical grouping must be supported by diagnosis coding and clinical documentation, making alignment between clinical notes and billing data essential.
Functional Level and Comorbidity Adjustment
PDGM incorporates functional status and comorbidity information to adjust payment based on patient complexity. Functional limitations and secondary diagnoses can increase reimbursement when accurately documented and supported.
This creates strong incentives for accurate assessment and documentation—but also increases audit sensitivity when documentation does not clearly support the assigned grouping.
PDGM and Documentation Sensitivity
PDGM is highly documentation-driven. Payment depends on whether clinical records support the assigned grouping, functional level, and comorbidity adjustments.
Operationally, this means HHAs must ensure:
- Consistent documentation across disciplines
- Alignment between OASIS responses and visit notes
- Accurate diagnosis capture without unsupported coding
Weak documentation is one of the most common causes of PDGM-related denials and reviews.
How PDGM (Patient-Driven Groupings Model) Works in Practice
In practice, PDGM reshapes home health operations by shifting the focus from visit volume to clinical accuracy, timing, and documentation alignment. Every Medicare home health episode is evaluated through the PDGM lens, making intake workflows, assessment accuracy, and interdisciplinary documentation central to payment and compliance.
Step 1: Referral Intake and Admission Classification
PDGM workflows begin at referral intake. HHAs must determine whether the admission is community-based or institutional, based on where the patient is coming from (e.g., hospital, IRF, SNF versus home).
Operationally, this requires:
- Accurate capture of referral source
- Verification of recent inpatient or post-acute stays
- Alignment between intake documentation and billing data
Admission source classification is a high-impact PDGM variable and a frequent source of payment error when intake workflows are inconsistent.
Step 2: Start of Care Assessment and OASIS Alignment
At start of care, clinicians complete the OASIS assessment and begin clinical documentation that establishes the patient’s functional level, clinical condition, and care needs.
In practice, this step determines much of the PDGM grouping logic. Agencies must ensure:
- OASIS responses are accurate and defensible
- Visit notes support reported functional limitations
- Diagnoses captured align with the primary reason for care
Misalignment between OASIS and clinical documentation is one of the most common triggers for PDGM-related reviews.
Step 3: Clinical Grouping and Diagnosis Capture
PDGM assigns patients to clinical groupings based on the primary reason for home health services. This grouping must be supported by diagnosis coding and clinical narrative.
Operationally, this requires close coordination between clinicians and coding or billing staff to ensure:
- The primary diagnosis reflects the true focus of care
- Secondary diagnoses are captured appropriately
- Documentation supports medical necessity and complexity
Over- or under-coding diagnoses can both create compliance risk under PDGM.
Step 4: Ongoing Documentation and Mid-Period Changes
Each 30-day PDGM payment period stands on its own. Changes in patient status, care needs, or diagnoses must be documented clearly within the period to support payment.
In practice, agencies must:
- Track clinical changes in real time
- Update documentation to reflect evolving needs
- Ensure interdisciplinary notes remain consistent
Failure to reflect changes within the correct payment period can result in lost reimbursement or audit exposure.
Step 5: Billing, Review, and Audit Readiness
Once the payment period ends, claims are submitted based on the PDGM grouping and documentation. Medicare and Medicare Advantage plans may review claims retrospectively.
Agencies with strong PDGM performance typically invest in:
- Pre-billing review of documentation alignment
- OASIS and diagnosis validation
- Internal audits focused on high-risk groupings
This proactive approach reduces denials and downstream compliance risk.
Billing and Reimbursement in PDGM
PDGM directly affects how Medicare home health services are reimbursed and reviewed. While it aims to better match payment to patient needs, it also increases sensitivity to documentation quality and operational consistency.
How PDGM Affects Medicare Home Health Reimbursement
Under PDGM, reimbursement is driven by patient characteristics rather than therapy volume. This means:
- Payment is determined early in the episode
- Documentation errors cannot be “offset” by visit volume
- Inaccurate grouping leads directly to under- or overpayment
For HHAs, this elevates the importance of front-end accuracy and mid-episode documentation discipline.
PDGM and Documentation-Driven Denial Risk
PDGM increases denial risk when documentation does not clearly support:
- Admission source classification
- Clinical grouping selection
- Functional level scoring
- Comorbidity adjustments
Because PDGM relies heavily on standardized data, even small inconsistencies can result in payment challenges during review.
System Limitations and Common PDGM Operational Challenges
Many PDGM issues stem from operational constraints, including:
- Fragmented intake systems that misclassify admission source
- Clinician training gaps on PDGM documentation implications
- Misalignment between OASIS and visit notes
- Limited QA capacity to review PDGM groupings before billing
- Delayed documentation, especially in the first days of care
Agencies that treat PDGM as an end-to-end workflow—rather than a billing afterthought—tend to perform better financially and compliantly.
How PDGM Influences Quality, Access, and Equity in Home Health
PDGM shapes not only reimbursement, but also how care is delivered and prioritized across patient populations.
PDGM and Quality of Home Health Care
When implemented well, PDGM can support quality by encouraging accurate assessment, appropriate care planning, and alignment of services with patient needs.
However, if documentation burden overwhelms clinical workflows, quality can suffer through rushed assessments or incomplete narratives.
PDGM and Access to Home Health Services
PDGM may influence access when agencies become cautious about admitting high-complexity patients due to documentation and audit risk.
Access challenges may be most pronounced for patients with multiple comorbidities, limited caregiver support, or unstable social conditions.
Equity Considerations Under PDGM
Equity risks arise if standardized grouping logic fails to capture social and environmental factors that affect care complexity. Agencies that contextualize PDGM documentation—without overstating clinical status—are better positioned to serve complex populations without increasing compliance exposure.
Frequently Asked Questions about PDGM
1. What is PDGM (Patient-Driven Groupings Model) in home health?
PDGM is Medicare’s home health payment model that determines reimbursement based on patient characteristics such as clinical condition, functional status, admission source, and comorbidities rather than therapy visit volume.
2. How does PDGM affect Medicare home health reimbursement?
PDGM assigns patients to payment groups that determine reimbursement for each 30-day period. Accurate documentation and assessment directly affect payment amounts.
3. What role does OASIS play in PDGM?
OASIS data is used to capture patient characteristics that feed PDGM grouping logic. Inconsistencies between OASIS and clinical documentation are a common source of PDGM denials.
4. Why is PDGM considered documentation-sensitive?
Because payment is based on standardized assessments and diagnoses, weak or inconsistent documentation can lead to underpayment, denials, or audits even when care delivery is appropriate.
5. What is admission source under PDGM and why does it matter?
Admission source indicates whether a patient is admitted from the community or an institutional setting. It directly affects reimbursement and is a frequent area of audit focus.
6. How do comorbidities affect PDGM payment?
Secondary diagnoses can increase reimbursement under PDGM when they reflect additional clinical complexity. These must be clearly documented and supported to avoid compliance risk.
7. Does PDGM apply to Medicare Advantage home health?
Medicare Advantage plans often mirror PDGM principles but may apply additional authorization, documentation, or utilization controls beyond Medicare fee-for-service rules.
8. What are common PDGM compliance and audit risks?
Common risks include misclassified admission source, unsupported diagnoses, inconsistent functional scoring, and misalignment between OASIS and visit notes.
