What is PHE (Public Health Emergency) in Healthcare?
A Public Health Emergency (PHE) is a formal government declaration that an event—such as an infectious disease outbreak, natural disaster, or other health threat—poses a significant risk to public health and requires emergency response measures. In U.S. healthcare, “PHE” most commonly refers to a federal public health emergency declaration that enables temporary policy changes across healthcare delivery, coverage, and reimbursement.
From an operational perspective, a PHE matters because it can unlock time-limited flexibilities that affect real-world workflows: telehealth rules, coverage requirements, cost-sharing, provider enrollment, licensing, reporting, and certain billing and documentation standards. These flexibilities can apply across Medicaid and Medicare and may also influence state rules and payer policies.
A PHE is not simply a public announcement—it is a policy switch. When a PHE is active, healthcare organizations often see rapid changes to what services can be delivered, how they are reimbursed, and how compliance expectations are applied. For clinics, health systems, payers, and vendors, understanding PHE policy is essential for building workflows that remain compliant as rules shift during and after the emergency.
Key Components of a Public Health Emergency (PHE)
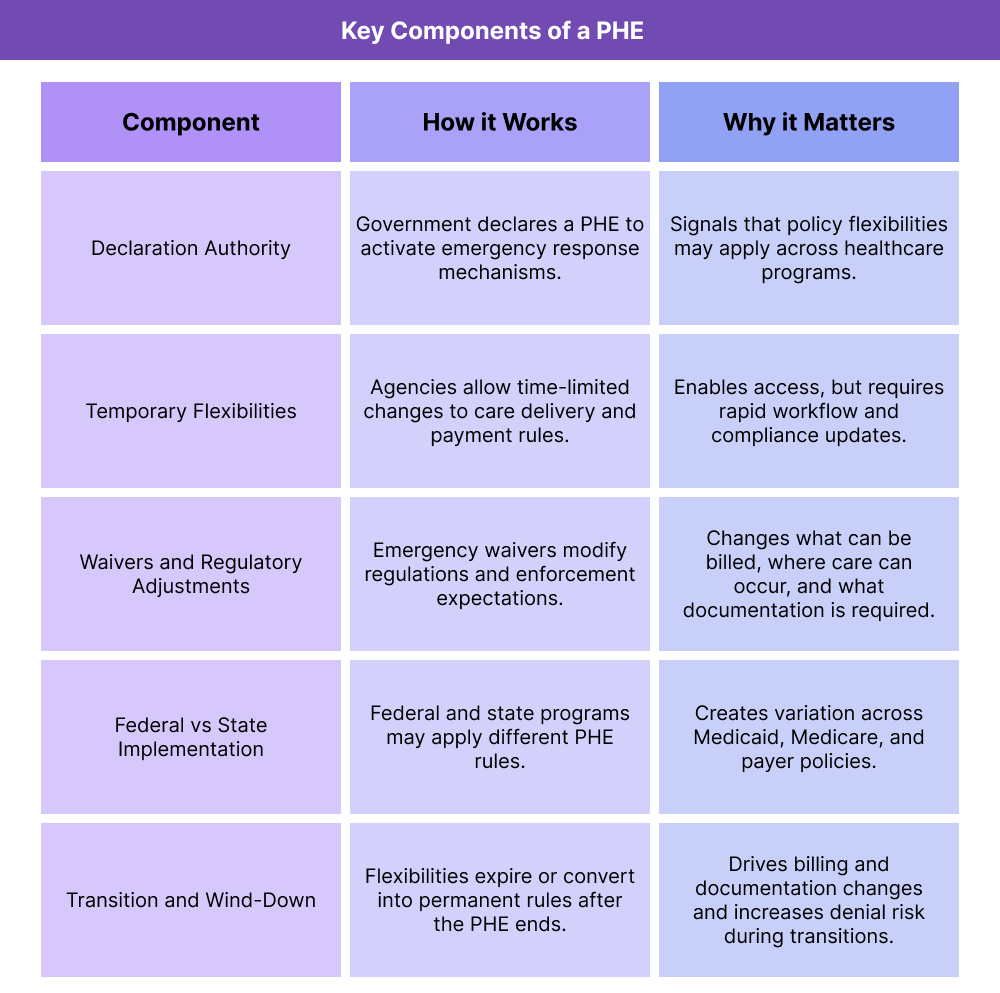
PHE declarations are often discussed broadly, but they are best understood through their operational components. Each component affects how care is delivered, how payment rules change, and how organizations manage compliance during a period of rapid policy adjustments.
PHE Declaration Authority and Trigger Events
A PHE is declared when government leaders determine that a situation poses a public health threat requiring coordinated response. Trigger events can include infectious disease outbreaks, severe disasters, or other emergent threats. The declaration establishes the legal and administrative basis for emergency actions.
Emergency Flexibilities and Temporary Policy Changes
During a PHE, agencies may allow temporary flexibilities that reduce barriers to care or support rapid scaling of services. These flexibilities often affect:
- Telehealth access and coverage rules
- Provider enrollment, credentialing, and licensing requirements
- Site-of-service rules and care delivery locations
- Coverage requirements and cost-sharing policies
- Reporting and documentation expectations
These changes are designed to improve access and continuity, but they also create operational complexity because rules can differ by payer and change quickly.
PHE Waivers and Regulatory Adjustments
Many PHE flexibilities are implemented through waivers or emergency regulatory adjustments. For healthcare organizations, this is where day-to-day practice changes: what can be billed, where it can be delivered, and what documentation standards apply.
State vs. Federal PHE Impacts
PHE impacts often differ across federal and state systems. Federal flexibilities may influence Medicare and broad federal guidance, while states may implement additional rules for Medicaid programs. This matters for organizations operating across multiple states, where PHE-driven changes may not be uniform.
PHE End Dates and Operational Transition
PHE changes are often time-limited, and the end of a PHE can trigger a return to pre-emergency rules or a shift into permanent policies. This transition period is often operationally challenging because organizations must update workflows, documentation, and billing logic quickly to avoid denials and compliance risks.
How a Public Health Emergency (PHE) Works in Practice in Healthcare
A Public Health Emergency (PHE) becomes “real” for healthcare organizations when policy and reimbursement rules change faster than normal operating cycles. In practice, PHE-driven changes cascade through clinical operations, billing, compliance, and reporting—often with different timelines and interpretations across Medicare, Medicaid, and managed care.
For providers and vendors, the challenge is not just understanding what changed, but operationalizing those changes safely: updating workflows, training teams, configuring systems, and then reversing or stabilizing those changes when the PHE winds down.
Step 1: A PHE Is Declared and Agencies Signal Immediate Priorities
Once a PHE is declared, agencies begin publishing emergency guidance and priorities. At this stage, organizations typically shift into a rapid-response posture:
- Monitoring payer and agency updates
- Identifying which service lines will be affected first (telehealth, inpatient, emergency, behavioral health)
- Assessing capacity constraints and access risks
- Establishing internal governance: “who decides, who updates workflows, who communicates changes”
This step is where operational maturity matters. Organizations with clear internal owners for compliance, billing, and clinical policy changes tend to adapt faster and with fewer downstream denials.
Step 2: Temporary Flexibilities Are Implemented Across Care Delivery and Payment
PHE flexibilities often focus on reducing friction so patients can access care and organizations can scale services. In practice, this commonly affects:
- Where care can be delivered (site-of-service flexibility)
- How care can be delivered (telehealth and virtual care expansion)
- Who can deliver care (temporary workforce and licensing accommodations)
- What documentation is required (temporary modifications or enforcement discretion)
- What payers cover and how quickly coverage rules change
For organizations, this step typically triggers:
- New visit types and scheduling workflows
- Adjustments to coding and billing processes
- Updates to templates and documentation guidance
- Changes to patient communications and eligibility guidance
This is also where system design becomes critical. If eligibility and billing rules are not reflected in practice management systems and EHR workflows, organizations can unintentionally create compliance risk while trying to expand access.
Step 3: States Operationalize PHE Rules Through Medicaid Policy and Systems
PHE impacts are rarely uniform across Medicaid. States may adopt federal flexibilities differently, implement additional state-level rules, or set their own timelines for changes.
Operationally, state implementation often requires updates to:
- Medicaid coverage and billing guidance
- Managed care policies and authorization workflows
- Claims and encounter edits within MMIS
- Data reporting requirements and quality program participation
This is where variation becomes a major risk. A workflow that is compliant in one state may be noncompliant in another if state Medicaid rules diverge. For multi-state organizations and vendors, the “PHE reality” is managing state-by-state differences while still delivering consistent care.
Step 4: Compliance and Oversight Expectations Shift During the Emergency
PHEs often create a new compliance landscape. Some requirements may be relaxed temporarily, while others become more scrutinized due to the increased risk of improper payments and rapid expansion of services.
In practice, this can mean:
- New billing patterns that attract audit attention later
- Documentation standards that change midstream
- Increased focus on fraud, waste, and abuse controls as services scale quickly
- Additional payer monitoring and retrospective reviews
This is where organizations should think ahead. Even when flexibility is allowed, maintaining strong documentation and clear rationale for services delivered helps reduce risk later—especially if oversight bodies review PHE-era billing after normal operations resume.
Step 5: The PHE Ends, and Organizations Transition to a New “Normal”
The wind-down period is often the hardest phase operationally. When a PHE ends, some flexibilities may expire immediately, others may be extended temporarily, and some may convert into permanent policy changes.
This transition requires organizations to:
- Update telehealth workflows and coverage rules
- Adjust documentation templates and billing guidance
- Reconfigure claims and encounter logic where needed
- Re-train staff on what has reverted versus what remains permanent
- Reassess denied claims and manage appeal/rework processes
For Medicaid organizations, wind-down can also involve eligibility shifts and coverage transitions that change patient access patterns. This can create operational strain and increase the need for care coordination support—especially for high-risk populations.
PHEs in Billing, Reimbursement, and System Limitations
A Public Health Emergency (PHE) can dramatically reshape billing and reimbursement rules in a short period. While these changes are intended to support access and continuity, they can also introduce inconsistency and denial risk—especially when rules differ across payers and states.
How a PHE Changes Healthcare Billing and Reimbursement
During a PHE, billing changes often occur in fast-moving waves. Common operational impacts include:
- Expanded telehealth billing and coverage rules
- Modified site-of-service requirements
- Temporary changes to supervision and provider eligibility rules
- Accelerated adoption of new codes, modifiers, and billing pathways
- Changes to prior authorization or utilization management workflows
The biggest revenue-cycle risk is misalignment between what staff believe is allowed and what payers will actually reimburse. During PHE periods, “policy updates” may be communicated through multiple channels, with timing delays between guidance and payer system implementation.
PHE Transitions Create Denial Risk and Rework
The end of a PHE frequently triggers reimbursement disruption. When flexibilities expire or shift, organizations can see:
- Denials for telehealth services that were previously covered
- Claims edits that revert to pre-PHE rules
- Confusion about documentation requirements
- Increased claim pend rates while payer systems adjust
For Medicaid, these risks are often amplified because state policies, managed care rules, and MMIS edits may not update in sync. If MMIS logic is updated later than clinical workflows, organizations can unknowingly submit claims under outdated assumptions.
System Limitations and PHE Operational Watch-Outs
PHE-era changes expose common system and process limitations:
- Workflow lag: clinical operations change before billing systems, causing mismatches
- Inconsistent templates: documentation tools not updated to reflect new requirements
- Eligibility complexity: coverage status changes faster than front-end verification processes
- Multi-payer variation: different rules across Medicare, Medicaid, and MCOs
- Retroactive reviews: payers may later audit whether PHE-era services met requirements
Organizations with strong governance, version control for policies, and centralized updates to documentation templates are more resilient during these transitions.
How PHEs Influence Quality, Access, and Equity in Healthcare
PHEs are often defined by rapid system change. Whether those changes improve or worsen equity depends on how flexibilities are implemented, communicated, and sustained.
Public Health Emergencies and Access to Care
PHE flexibilities are often designed to preserve access when in-person care is disrupted. Expanded telehealth, relaxed site requirements, and temporary changes to workforce rules can help patients maintain continuity.
However, access improvements are not evenly distributed. Patients without reliable internet, stable housing, transportation, or digital literacy may still face barriers—especially if health systems rely heavily on virtual-first models without alternative pathways.
Public Health Emergencies and Healthcare Quality
During a PHE, healthcare organizations often shift to crisis-mode operations. Quality programs may pause or evolve, and care teams may re-prioritize services based on urgency and capacity.
Quality impacts commonly include:
- Delayed preventive care and chronic disease follow-up
- Disruptions in behavioral health and SUD services
- Reduced care continuity due to staffing and access constraints
- Increased need for transitions-of-care management after hospitalizations
Organizations that maintain structured follow-up workflows, patient outreach, and clear documentation tend to protect quality more effectively during these periods.
Public Health Emergencies and Equity in Healthcare
PHEs often amplify existing inequities. Vulnerable populations are more likely to experience care disruptions, financial instability, and barriers to accessing new models of care.
Equity-sensitive approaches during a PHE often include:
- Multiple access pathways (telehealth plus in-person options)
- Outreach workflows for high-risk members
- Clear patient communications in culturally and linguistically appropriate formats
- Care coordination support for patients affected by coverage changes
When emergency flexibilities are treated as purely technical policy changes, inequities can deepen. When they are paired with thoughtful access design and care coordination, PHE changes can create lasting improvements—especially if effective flexibilities become permanent.
Frequently Asked Questions about PHE
1. What is a PHE (Public Health Emergency) in healthcare?
A Public Health Emergency (PHE) is a formal government declaration that a serious health threat requires emergency response measures. In healthcare operations, a PHE typically triggers temporary policy flexibilities that affect coverage, telehealth, billing, reporting, and compliance across Medicaid, Medicare, and payer programs.
2. What does a PHE declaration change for healthcare providers?
A PHE can change how and where providers deliver care, what services payers cover, and which billing and documentation requirements apply. Common operational changes include telehealth expansion, modified site-of-service rules, temporary workforce flexibilities, and shifts in utilization management policies.
3. How does a PHE affect telehealth coverage and billing?
During a PHE, telehealth rules are often expanded to support access when in-person care is limited. This can include broader coverage, relaxed location requirements, and new billing pathways. Providers still need to align workflows to payer-specific rules, which can vary across Medicaid, Medicare, and managed care plans.
4. How does a PHE affect Medicaid programs and managed care plans?
PHE impacts in Medicaid often depend on state implementation. States and managed care organizations may issue specific coverage guidance, modify authorization requirements, and update MMIS edits. Because timelines and rules can differ by state, multi-state organizations often need state-specific workflows during a PHE.
5. Why does the end of a PHE create billing and reimbursement risk?
When a PHE ends, temporary flexibilities may expire or shift into new permanent policies. This can create denials if organizations continue billing under outdated rules, especially for telehealth, site-of-service requirements, or documentation standards. Transition periods often require rapid updates to templates, coding guidance, and staff training.
6. How do healthcare organizations stay compliant during a PHE?
Strong compliance during a PHE depends on clear internal governance, rapid policy monitoring, consistent documentation standards, and system updates that keep billing workflows aligned with payer rules. Even when flexibilities are allowed, maintaining audit-ready documentation helps reduce risk later.
7. How does a PHE influence quality of care and care coordination?
PHEs can disrupt preventive care, chronic condition follow-up, behavioral health access, and transitions of care. Organizations that maintain structured outreach and care coordination workflows are better positioned to protect quality during emergency periods.
8. How does a PHE affect access and equity in healthcare?
PHE flexibilities can improve access for many patients, but they can also widen inequities for individuals who lack internet access, transportation, stable housing, or digital literacy. Equity-sensitive operations typically include multiple care access pathways, proactive outreach, and culturally appropriate patient communications.
9. Are PHE flexibilities permanent?
Most PHE flexibilities are temporary, but some may be extended or converted into permanent policy depending on federal and state decisions. Organizations should plan for change by tracking which flexibilities are time-limited versus adopted into standard practice.
