What is MBQIP (Medicare Beneficiary Quality Improvement Project)?)
The Medicare Beneficiary Quality Improvement Project (MBQIP) is a national quality reporting and improvement initiative focused on Critical Access Hospitals (CAHs). MBQIP helps rural hospitals measure care performance using a standardized core set of quality measures, then use that data to drive targeted improvement over time.
MBQIP operates through the Medicare Rural Hospital Flexibility (Flex) Program. Participating states and CAHs report on a shared measure set that reflects the realities of low-volume rural hospitals, including emergency department performance, patient safety, and patient experience. The goal is to strengthen rural quality infrastructure and ensure CAHs can demonstrate measurable quality outcomes alongside larger hospital systems.
In practice, MBQIP is both a reporting framework and an improvement engine. By collecting consistent data across CAHs, MBQIP enables benchmarking, identifies system-wide rural care risks, and supports performance improvement work that protects quality, access, and reimbursement in rural communities.
Key Components of an MBQIP
MBQIP is built around a standardized “core measure set” that Critical Access Hospitals (CAHs) report through the Flex Program. The measure set is intentionally aligned to national quality standards, but tailored to rural hospital realities such as low patient volumes, limited specialty coverage, and heavy reliance on emergency and outpatient services.
MBQIP’s structure centers on two things: a defined group of measure domains that CAHs report consistently, and an improvement expectation that hospitals use those results to select priorities and run performance work over time.
MBQIP Core Measure Reporting
CAHs participating in MBQIP report a core set of quality measures each year. These measures are selected through a national process involving State Flex Programs, CAHs, and federal rural health policy leaders. The goal is not only reporting for compliance, but creating consistent benchmarking across rural hospitals.
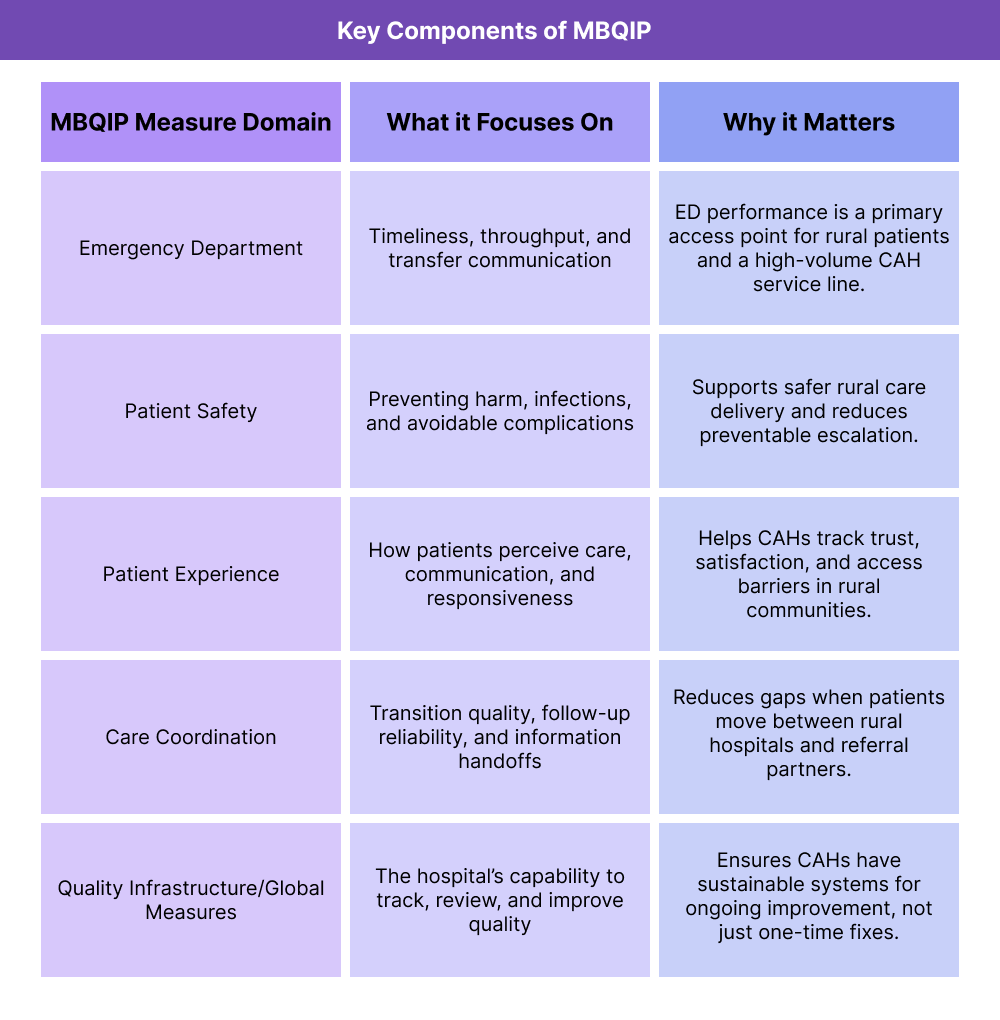
MBQIP Measure Domains
MBQIP measures are organized into domains that reflect high-impact rural care priorities. While the exact measures can evolve year to year, MBQIP consistently focuses on performance areas like emergency department care, patient safety, patient experience, care coordination, and overall quality infrastructure.
Using MBQIP Data for Improvement
MBQIP expects CAHs to go beyond submission and use results to drive improvement. Hospitals review domain performance, identify gaps that matter most locally, and build targeted quality improvement activities around those risks. This is what transforms MBQIP from a reporting list into a continuous improvement engine.
How MBQIP Works in Practice
MBQIP functions as a structured quality cycle for Critical Access Hospitals (CAHs): report a standardized measure set, review performance, identify rural-relevant gaps, and implement improvement actions through local and state Flex Program support. The intent is to make quality measurement usable and sustainable for low-volume rural hospitals.
Step 1: CAHs Collect and Report MBQIP Measures
Participating CAHs gather data for the MBQIP core measure set using their existing clinical, operational, and patient experience workflows. Measures are reported through the state Flex Program on a recurring schedule. Reporting creates a consistent baseline across CAHs and allows performance to be compared over time.
Step 2: State Flex Programs Aggregate and Benchmark Results
State Flex Programs compile CAH submissions and provide benchmarking, coaching, and technical assistance. This structure helps rural hospitals interpret results in context and understand where they are performing strongly versus where gaps may be emerging.
Step 3: CAHs Identify Improvement Priorities From MBQIP Data
Hospitals review their domain results to determine which areas are most urgent or high-impact locally. Priorities may be driven by safety events, emergency department throughput, transfer patterns, or patient experience signals. The key is that priorities are evidence-based rather than anecdotal.
Step 4: Improvement Work Is Implemented and Re-Measured
After selecting priority areas, CAHs implement improvement actions—often in partnership with state Flex support or rural quality collaboratives. Progress is tracked through repeat measure reporting, allowing hospitals to verify whether changes are working and to sustain gains over time.
MBQIP in Billing, Reimbursement, and System Limitations
MBQIP is not a billing program, but it affects reimbursement stability for rural hospitals because it supports the quality infrastructure tied to Medicare participation, public reporting, and value-based accountability. For a Critical Access Hospital (CAH), MBQIP helps ensure that core care processes—especially in the emergency department—are measured and improved consistently, which protects long-term certification and payer confidence.
How MBQIP Supports Reimbursement Readiness for CAHs
MBQIP measure reporting helps CAHs demonstrate that they are actively monitoring and improving care quality. This matters because rural hospitals must maintain survey readiness and quality oversight capacity to remain Medicare-participating providers. Strong MBQIP performance signals operational reliability in areas Medicare and other payers scrutinize, including patient safety and patient experience.
MBQIP data also supports rural benchmarking, allowing CAHs to show improvement trends even when low volume makes year-to-year variability harder to interpret in isolation.
Where MBQIP Intersects With Payer Expectations
While MBQIP is administered through the Flex Program, the measures align with broader national quality expectations. Consistent MBQIP participation helps CAHs maintain readiness for:
- Federal quality reporting requirements tied to hospital participation
- Payer quality program reviews in rural network contracting
- Performance improvement documentation during surveys or audits
In short, MBQIP helps rural hospitals stay compliant and defensible in reimbursement environments that increasingly require measurable quality oversight.
System Limitations and Operational Watch-Outs
MBQIP is designed for rural realities, but practical limitations still exist:
- Low patient volume can cause performance swings that require trend-based interpretation
- Data collection may depend on manual workflows if CAHs lack strong reporting systems
- Some measure domains may feel misaligned with a specific CAH’s service mix
- Reporting alone does not improve performance unless hospitals run real improvement work
Technology can reduce burden by streamlining measure capture and tracking, but MBQIP success ultimately depends on local follow-through on identified gaps.
How MBQIP Influences Quality, Access, and Equity in Healthcare
MBQIP exists because rural hospitals face unique quality and access pressures. By standardizing quality measures for CAHs and supporting continuous improvement, MBQIP strengthens care in communities where hospital services are limited and alternatives are often far away.
Quality and Safety Improvements Through MBQIP
MBQIP helps CAHs focus improvement work on high-impact rural domains such as emergency department performance, patient safety, and care coordination. When these areas improve, rural hospitals reduce preventable escalations, improve clinical reliability, and strengthen continuity for patients who may otherwise experience fragmented care.
Over time, consistent MBQIP use builds a sustained quality culture rather than one-off project work.
Access Implications for Rural Communities
For many rural regions, the local CAH is the primary—or only—hospital access point. MBQIP supports access by helping these hospitals remain strong, compliant, and operationally stable. Improvements in emergency department throughput, transfer communication, and safety help patients receive timely care locally and reduce avoidable travel or delays.
Equity Benefits of Rural Quality Measurement
Rural populations often face higher chronic disease burden, transportation barriers, and fewer specialty options. MBQIP supports equity by ensuring rural hospitals have a structured, national-quality framework that is realistic for CAH environments. This helps reduce quality gaps between rural and urban care settings and strengthens outcomes for communities that are historically underserved.
Frequently Asked Questions about MBQIP
1. What is MBQIP (Medicare Beneficiary Quality Improvement Project)?
MBQIP is a national quality reporting and improvement initiative for Critical Access Hospitals (CAHs) that uses a standardized rural-focused measure set to drive continuous care improvement.
2. Who participates in MBQIP?
MBQIP is designed for Critical Access Hospitals. Participation occurs through state Medicare Rural Hospital Flexibility (Flex) Programs, which coordinate reporting and improvement support.
3. What does MBQIP measure?
MBQIP measures performance across domains such as emergency department care, patient safety, patient experience, care coordination, and overall quality infrastructure. The specific core measures may evolve, but the domains stay focused on rural hospital priorities.
4. Is MBQIP mandatory for Critical Access Hospitals?
MBQIP participation is not federally mandatory in the same way some hospital programs are, but it is the primary national quality framework used by CAHs through the Flex Program. Many CAHs participate to meet rural quality expectations and support survey readiness.
5. How does MBQIP data get used?
CAHs report MBQIP measures, review results with state Flex support, identify priority gaps, and run local performance improvement work. Reporting is intended to lead to measurable improvement, not just compliance.
6. Why is MBQIP important for rural hospitals?
MBQIP gives CAHs a realistic, standardized way to benchmark and improve quality in low-volume rural settings. It strengthens safety, emergency performance, and continuity in communities where hospital access is limited.
7. How is MBQIP different from other hospital quality programs?
MBQIP is tailored specifically to CAH environments and rural care realities, while many other hospital quality programs are built around higher-volume acute hospital models. MBQIP emphasizes a manageable rural measure set paired with improvement support through the Flex Program.
8. How does MBQIP relate to Rural Health Clinics (RHCs)?
MBQIP focuses on Critical Access Hospitals, while Rural Health Clinics (RHCs) are outpatient clinics certified to improve access to primary care in rural areas. Both are part of the rural care ecosystem and often serve overlapping communities, but they operate under different certification models, service scopes, and quality reporting structures.
