What is Targeted Probe and Educate (TPE)?
Targeted Probe and Educate (TPE) is a Medicare medical review program conducted by Medicare Administrative Contractors (MACs) to evaluate provider billing accuracy, identify improper payment risks, and reduce recurring documentation or coding errors.
Unlike broad federal audits, TPE focuses narrowly on specific services or providers showing billing practices that differ from peers, exhibit high denial rates, or fail to meet requirements outlined in Local Coverage Determinations (LCDs), National Coverage Determinations (NCDs), or CMS policy.
TPE reviews occur in up to three rounds, each involving:
- A probe sample of claims
- A thorough medical record review
- An individualized education session between the MAC and provider
- A period for corrective action before any subsequent round
Most providers successfully resolve issues during the first round, preventing further review and avoiding escalation to broader audit programs.
TPE is designed to be corrective, not punitive. Its primary purpose is to help providers understand and meet Medicare requirements by clarifying documentation standards, coding expectations, and clinical criteria necessary for payment.
However, failure to correct identified errors may result in extrapolated overpayments, 100% prepayment review, or referral to other integrity contractors such as UPICs.
TPE is commonly initiated for services with:
- High national error rates
- Inconsistent medical necessity documentation
- Frequent LCD/NCD-related issues
- Aberrant billing compared to local or national benchmarks
- Ongoing denials not corrected through provider outreach
By pairing targeted audits with provider-specific education, TPE strengthens Medicare program integrity while supporting compliant, sustainable billing practices for healthcare organizations.
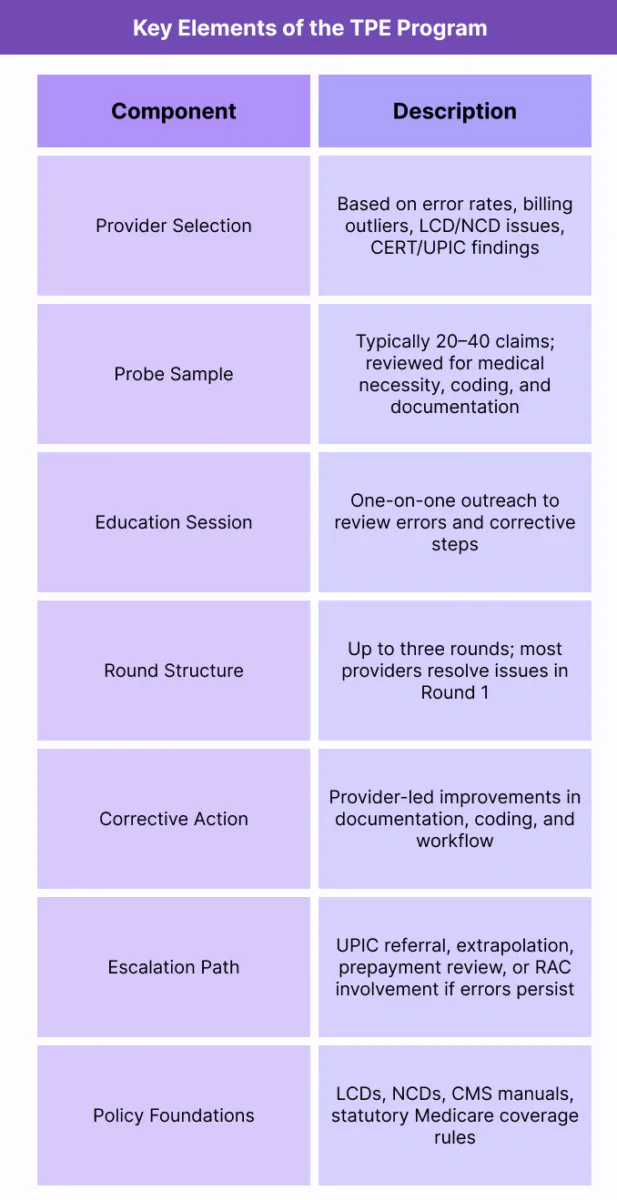
Key Components of Targeted Probe and Educate (TPE)
Targeted Probe and Educate (TPE) is a structured medical review program used by Medicare Administrative Contractors (MACs) to evaluate provider compliance, identify billing errors, and reduce improper payments.
TPE relies on a defined, repeatable workflow that emphasizes education-first correction, ensuring providers understand Medicare’s clinical, documentation, and coding requirements before more serious audit actions are taken.
1. Provider and Service Selection Criteria
- MACs select providers or services for TPE based on:
- High denial rates compared to peers
- Billing patterns inconsistent with national or regional norms
- Frequent errors related to LCD or NCD requirements
- CERT, UPIC, or OIG findings indicating potential vulnerabilities
- Rapid growth in service volume or unusual utilization trends
- Selection is data-driven and typically focuses on high-risk codes, benefit categories, or historically problematic services.
2. Probe Sample and Medical Review
- Each round begins with a probe sample—usually 20–40 claims—chosen to reflect recent billing behavior.
- MAC reviewers assess:
- Medical necessity
- Documentation sufficiency
- Compliance with LCD/NCD criteria
- Coding accuracy and modifier usage
- Beneficiary eligibility
- Frequency limitations and statutory constraints
- Errors in the probe sample determine whether education or further review is required.
3. Education Session and Corrective Action
- After reviewing the sample, the MAC holds a one-on-one education session with the provider or billing team.
- These sessions focus on:
- Identified error trends
- Required clinical documentation elements
- Coding corrections and modifier guidance
- LCD/NCD interpretation
- Steps for improvement before the next round
- Providers are given time to implement corrective actions before another probe occurs.
4. Three-Round Review Structure
- TPE includes up to three rounds, each building on the last:
- Round 1: Initial review + education
- Round 2: Follow-up review for improvement
- Round 3: Final review if significant errors persist
- Most providers complete the program after Round 1, especially when corrective steps are applied promptly.
5. Potential Outcomes and Escalation
- If error rates remain high after three rounds, MACs may:
- Refer the provider to UPICs for fraud or abuse investigation
- Initiate 100% prepayment review
- Apply extrapolated overpayments
- Refer cases to RAC or OIG as appropriate
- These escalations shift the review from educational to enforcement-based.
6. Interaction With LCDs, NCDs, and Other Medicare Policies
- TPE is heavily anchored in existing coverage frameworks:
- LCDs drive many TPE determinations, especially for specialty services
- NCDs govern national medical necessity and documentation expectations
- CMS manuals and statutes are applied for benefit category issues
- Understanding these policies is essential for compliance during any TPE review.
7. Compliance and Revenue Cycle Implications
- Effective TPE management supports:
- Lower denial rates
- Improved documentation quality
- Faster reimbursement
- Fewer post-payment recoupments
- Reduced audit exposure
- Stronger internal compliance programs
- Organizations with standardized documentation protocols are more likely to exit TPE early and avoid further scrutiny.
How Targeted Probe and Educate (TPE) Works in Practice
Targeted Probe and Educate (TPE) is one of the most operationally impactful Medicare review processes providers encounter.
Unlike RAC or UPIC audits, TPE is highly interactive, corrective, and education-driven, requiring close coordination between clinicians, coding teams, billing departments, and compliance leaders.
A TPE review typically unfolds across a predictable set of operational steps, from the initial MAC notification through probe sampling, education, corrective action, and—if necessary—subsequent rounds.
Step 1: Receiving the TPE Notification Letter
- A provider begins the TPE process when the assigned Medicare Administrative Contractor (MAC) issues an official TPE Notification Letter, which includes:
- The CPT®/HCPCS code(s) or service category under review
- The reason for selection (e.g., high denial rate, LCD errors, aberrant utilization)
- Instructions for medical record submission
- Timelines and documentation requirements
- Compliance and billing teams should immediately:
- Assign internal ownership
- Notify involved clinicians
- Review relevant LCDs/NCDs
- Begin preparing medical records and documentation
- Timing is critical—failure to submit documentation promptly may result in automatic denials.
Step 2: Preparing and Submitting Medical Records
- Providers must submit a complete set of medical records for each claim in the MAC’s probe sample (usually 20–40 claims).
- A thorough submission typically includes:
- Progress notes and clinical documentation
- Orders, referrals, or prior test results
- Diagnoses supporting medical necessity
- Procedure reports, imaging results, or test interpretations
- Proof of practitioner signatures and credentials
- Correct CPT/HCPCS and ICD-10 coding alignment
- Any LCD- or NCD-specific documentation elements
- Billing and compliance staff work together to ensure every element required by CMS policy is present.
Step 3: MAC Medical Review and Error Identification
- MAC reviewers then evaluate each claim in the probe sample for:
- Compliance with LCD/NCD criteria
- Accuracy of CPT®/HCPCS and ICD-10 coding
- Documentation sufficiency
- Medical necessity and clinical rationale
- Frequency limitations
- Correct modifier usage
- Statutory or benefit category restrictions
- MACs issue preliminary findings summarizing:
- Error types (e.g., missing documentation, invalid diagnoses, medical necessity issues)
- Error frequency
- Root causes
- These findings guide the provider-specific education session.
Step 4: Provider-Specific Education Session
- The education session is the defining feature of the TPE program.
- During this one-on-one meeting, MAC educators review:
- Each category of error
- Relevant coverage policies behind the denial
- Required documentation elements
- Proper coding, modifier usage, or clinical criteria
- Steps to avoid errors in subsequent rounds
- Education sessions are collaborative and constructive, not adversarial.
- CMS explicitly instructs MACs to focus on teaching, not penalizing.
Step 5: Corrective Action Implementation
- After the education session, providers are given time to implement improvements such as:
- Updating documentation templates
- Revising intake or clinical workflows
- Strengthening medical necessity explanations
- Re-training clinicians or billers
- Adjusting internal coding practices
- Adding LCD/NCD prompts to EHR systems
- Conducting internal audits before claim submission
- Organizations that adopt rapid corrective action tend to resolve TPE issues in Round 1.
Step 6: Follow-Up Probe Review (Round 2 or Round 3, if needed)
- If errors persist, MACs move to:
- Round 2 (second probe sample + education)
- Round 3 (final opportunity to demonstrate improvement)
- Improvement is measured by:
- Lower error rates
- Better medical necessity documentation
- Correct diagnosis and procedure codes
- Adherence to LCD/NCD requirements
- Failure to improve triggers escalation.
Step 7: Escalation Outcomes if Errors Remain High
- If the provider does not demonstrate adequate improvement after three rounds, the MAC may escalate to:
- UPIC referral (fraud/waste/abuse investigation)
- 100% prepayment review
- Extrapolated overpayment calculations
- RAC referral for further review
- CMS-directed corrective action plans
- At this point, TPE shifts from an educational initiative to an enforcement action.
Step 8: Integration Into Long-Term Compliance Programs
- Organizations incorporate TPE lessons into ongoing compliance by:
- Conducting periodic self-audits
- Reviewing LCDs/NCDs regularly
- Updating templates, checklists, and intake forms
- Training clinicians on medical necessity documentation
- Monitoring denial patterns to detect emerging risks
- Including TPE risk areas in annual compliance plans
- Effective TPE management strengthens internal governance and reduces future audit exposure.
TPE in Medicaid Billing, Reimbursement, and Fiscal Limitations
Targeted Probe and Educate (TPE) directly affects reimbursement operations because it evaluates the accuracy, sufficiency, and medical necessity of claims that providers submit to Medicare.
While TPE is designed to be educational rather than punitive, it can still lead to significant payment delays, increased denial rates, and long-term audit exposure when providers do not fully meet Medicare requirements.
TPE functions as both a corrective tool and a compliance checkpoint, making it one of the most influential components of Medicare’s payment integrity strategy.
How TPE Influences Billing and Reimbursement
- TPE can impact revenue in several ways:
- Delayed payments due to record submission and review timelines
- Temporary cash-flow disruption when large sets of claims undergo medical review
- Increased administrative load for documentation preparation
- Potential denial of high-dollar services if documentation does not support medical necessity
- Reprocessing timelines when providers must rebill corrected claims
- Because TPE reviews documentation against LCDs, NCDs, CMS manuals, and statutory requirements, even minor lapses (e.g., missing signatures, insufficient clinical details) can result in denials.
Error Categories That Commonly Lead to Denials
- Frequent TPE errors include:
- Missing or incomplete clinical notes
- ICD-10 codes that do not support medical necessity
- Lack of documentation required by the relevant LCD/NCD
- Incorrect or missing modifiers
- Signature or credential issues
- Failure to show progression, medical rationale, or prior conservative therapy
- Missing test orders or plan-of-care elements
- These errors not only impact TPE outcomes but contribute to long-term denial trends if not corrected.
Operational Burden and Documentation Demands
- TPE can create significant operational strain:
- Short turnaround timelines for medical record submission
- Extensive cross-department coordination (clinical, HIM, RCM, compliance)
- Need to retrieve complete records rather than partial extracts
- Risk of inconsistent documentation across providers within the same organization
- Additional workload for appeals and follow-up
- Organizations with incomplete or decentralized record systems often struggle during Round 1 and Round 2 of TPE.
Limitations in Education and Interpretation
- While TPE is designed to be educational, challenges may arise:
- Education sessions vary in depth depending on the MAC
- LCD interpretations may differ subtly from MAC to MAC
- Some services have no LCD, forcing MACs to rely on broader CMS rules
- TPE reviewers may focus heavily on documentation rather than clinical judgment
- Providers sometimes receive high-level guidance but lack service-specific examples
- This can leave providers with lingering uncertainty about how to avoid future denials.
Impact on Large or Multi-State Organizations
- Multi-site and multi-state organizations face unique limitations:
- Different MACs may initiate TPE on the same service with slightly different expectations
- Cross-jurisdiction LCD variation adds complexity
- Internal standardization becomes difficult when documentation templates must satisfy multiple contractors
- Higher audit exposure due to large claim volumes
- These factors increase administrative intensity and slow reimbursement cycles.
Escalation Risks and Financial Exposure
- Failure to correct issues by Round 3 may result in:
- Extrapolated overpayments
- 100% prepayment review, severely delaying cash flow
- UPIC referral for potential fraud/waste/abuse
- RAC involvement
- Long-term monitoring by the MAC
- These outcomes transform TPE from an educational process to a significant financial and compliance risk.
Key Takeaway
TPE plays a crucial role in Medicare’s payment integrity ecosystem.
When managed proactively—with strong documentation workflows, LCD/NCD literacy, and rapid corrective action—TPE can be completed quickly and painlessly.
However, when documentation gaps persist, TPE becomes a major bottleneck for cash flow, claim accuracy, and long-term audit risk.
How TPE Influences Quality, Access, and Equity in Medicaid Financing
Although Targeted Probe and Educate (TPE) is framed primarily as a medical review and education program, its real-world impact extends far beyond billing accuracy.
TPE shapes how consistently Medicare rules are applied across regions, how equitably providers experience administrative oversight, and how effectively documentation standards are upheld across the healthcare system.
By correcting documentation and medical necessity deficiencies, TPE supports proper payment and reduces systematic claim variation. However, its implementation also raises considerations related to administrative equity, practice burden, and access—particularly among smaller, rural, or resource-constrained providers.
Promoting Consistency in Documentation and Medical Necessity Standards
- TPE strengthens national consistency by:
- Requiring uniform adherence to LCD/NCD requirements across all providers
- Reducing variability in how medical necessity is documented
- Identifying repeatable patterns of insufficient clinical detail
- Reinforcing CMS’s expectations for beneficiary eligibility, coding, and service rationale
- By standardizing the quality of documentation, TPE improves the reliability of Medicare claim adjudication and reduces improper payments.
Improving Care Quality Through Better Clinical Documentation
- High-quality documentation is directly tied to clinical quality.
- TPE-driven improvements often result in:
- Clearer treatment rationales
- Better capture of disease severity
- Improved continuity of care across providers
- More accurate diagnosis coding
- More defensible clinical decision-making
- These improvements enhance both the clinical record and downstream outcomes such as care coordination, risk adjustment accuracy, and patient safety.
Supporting Program Integrity and National Payment Accuracy
- TPE plays an important role in Medicare’s improper payment reduction strategy:
- Identifying systemic documentation errors
- Reducing overuse of services lacking medical necessity
- Reinforcing appropriate utilization patterns
- Ensuring public funds are used responsibly
- By correcting issues early, TPE helps prevent larger-scale recoupments, audits, and enforcement actions.
Administrative Burden and Equity Considerations
- While TPE supports quality and consistency, its operational burden may fall unevenly across provider types.
- Smaller, rural, or understaffed organizations may struggle with:
- Tight documentation submission deadlines
- Limited administrative capacity
- Lack of dedicated compliance or HIM teams
- Less familiarity with complex LCD/NCD requirements
- Higher vulnerability to data-driven targeting due to low claim volume variability
- This can create administrative inequities, where providers with fewer resources face a disproportionate challenge in meeting TPE requirements.
Potential for Regional Variation Despite National Structure
- Even though all MACs follow CMS rules, regional differences may influence TPE experiences:
- Variability in MAC education quality
- Different LCD interpretations or emphasis areas
- Differences in what documentation is considered sufficient
- Variation in escalation thresholds after Round 1 or Round 2
- These differences can impact provider perception of fairness and administrative burden.
Impact on Access and Provider Participation
- TPE can indirectly affect beneficiary access:
- Practices overwhelmed by repeated TPE rounds may reduce Medicare service offerings.
- High documentation burden may discourage small or solo practices from participating in certain high-risk benefit categories.
- Frequent reviews can strain rural or safety-net providers serving vulnerable populations.
- Ensuring administrative processes do not unintentionally limit access is central to CMS’s health equity strategy.
Role in Advancing Transparency and Education-Driven Oversight
- TPE helps strengthen Medicare transparency and fairness by:
- Providing one-on-one education instead of punitive enforcement
- Clearly explaining coverage rules and required documentation
- Giving providers opportunities to correct issues before escalation
- Promoting a collaborative, rather than adversarial, oversight model
- This aligns with CMS’s shift toward educational intervention, reducing punitive measures unless necessary.
Key Insight
TPE enhances quality, accuracy, and compliance across the Medicare ecosystem by improving provider documentation, reducing improper payments, and standardizing claim expectations.
However, the administrative demands of TPE can disproportionately affect providers with fewer resources, making equitable implementation and clear education essential to ensure that oversight strengthens—rather than hinders—access to care.
Frequently Asked Questions about TPE
1. What is a Targeted Probe and Educate (TPE) review?
A TPE review is a Medicare medical review process conducted by MACs to evaluate a provider’s claims for medical necessity, documentation sufficiency, and billing accuracy.
It includes a probe sample of 20–40 claims, a detailed medical record review, and a one-on-one education session to help providers correct identified errors.
2. How are providers selected for TPE?
Providers are chosen based on data-driven indicators such as:
- High denial rates
- Billing patterns inconsistent with peers
- Errors related to LCD/NCD criteria
- CERT or UPIC findings
- Rapid growth in service volume
- Historically high improper payment risk
Selection is not random—it targets documented vulnerabilities.
3. What documentation is required for a TPE review?
Documentation must fully support medical necessity, coding accuracy, and coverage criteria, including:
- Clinical notes and progress documentation
- Orders, referrals, and test results
- Diagnoses supporting ICD-10 coding
- LCD/NCD-specific requirements
- Signatures and provider credentials
- Procedure reports, imaging, labs, or therapy notes
Incomplete documentation is the leading cause of TPE denials.
4. How many rounds are in the TPE process?
TPE includes up to three rounds:
- Round 1: Probe sample + education
- Round 2: Follow-up review if errors persist
- Round 3: Final review to assess improvement
Most providers resolve issues in Round 1 after implementing corrective actions.
5. What happens if providers fail TPE after all three rounds?
If error rates remain high, MACs may escalate to:
- UPIC referral for suspected fraud, waste, or abuse
- 100% prepayment review
- Extrapolated overpayments
- Referral to RAC or CMS for further action
At this point, TPE becomes an enforcement mechanism rather than an educational one.
6. How long does a TPE review take?
Timelines vary, but typically:
- Record submission: 30 days
- MAC review of probe sample: 30–60 days
- Education session: within weeks of findings
- Corrective action window: ~45–90 days
- Subsequent rounds follow a similar pattern
The full process may take several months if multiple rounds are required.
7. What’s the difference between TPE and RAC/UPIC audits?
TPE is corrective and educational, with individualized instruction and opportunities to improve.
RAC audits focus on improper payments and may involve extrapolation.
UPIC investigations address potential fraud or abuse and can lead to enforcement actions.
TPE is considered a gentler, collaborative review—unless errors persist, triggering escalation.
8. How can providers avoid future TPE reviews?
Key strategies include:
- Consistent adherence to LCD/NCD criteria
- Strong internal documentation templates
- Regular coding and compliance audits
- Staff training on medical necessity requirements
- Monitoring denial trends
- Ensuring accurate modifier and ICD-10 usage
Proactive compliance greatly decreases TPE selection risk.
