What Are Disproportionate Share Hospital (DSH) Payments?
Disproportionate Share Hospital (DSH) Payments are federal Medicaid adjustments that provide supplemental reimbursement to hospitals serving a high volume of low-income and uninsured patients. Authorized under Section 1923 of the Social Security Act, DSH payments help offset uncompensated-care costs and sustain safety-net providers essential to Medicaid access.
Each state receives an annual DSH allotment from the Centers for Medicare & Medicaid Services (CMS), which caps the total federal funds available for this purpose. States, in turn, allocate payments to qualifying hospitals through State Plan Amendments (SPAs) that define eligibility criteria, payment formulas, and reporting processes.
DSH is distinct from the Upper Payment Limit (UPL) program: while UPL ensures total Medicaid reimbursement does not exceed Medicare-equivalent ceilings, DSH specifically targets hospitals with disproportionate Medicaid and charity-care burdens. Both mechanisms operate under CMS oversight and are central to maintaining equitable hospital financing within Medicaid.
Participation in DSH requires hospitals to meet defined low-income utilization thresholds and submit annual cost reports documenting uncompensated-care levels. CMS audits and verifies these data to confirm compliance with federal funding limits and prevent duplication of payments with other Medicaid supplements such as Intergovernmental Transfers (IGTs) or Certified Public Expenditures (CPEs).
By directing funds toward financially vulnerable institutions, DSH payments support care continuity, access stability, and equity in the Medicaid system, ensuring that essential hospitals can continue to serve high-need populations despite below-cost reimbursement rates.
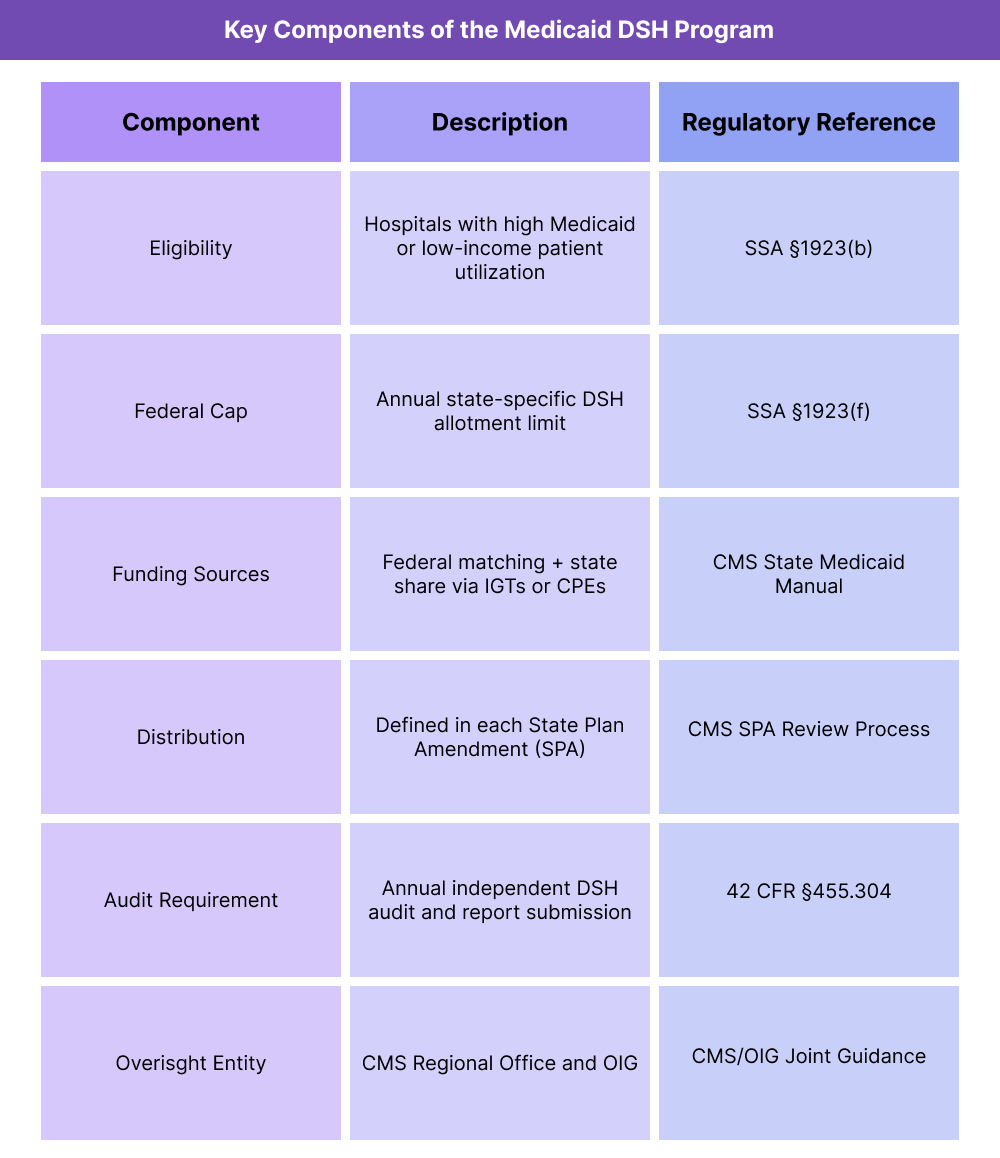
Key Components of Disproportionate Share Hospital (DSH) Payments
The Disproportionate Share Hospital (DSH) program is a cornerstone of Medicaid hospital financing, designed to protect hospitals that serve large volumes of low-income and uninsured patients. DSH combines federal and state funding streams to stabilize safety-net care and maintain access in communities with high Medicaid dependency.
Administered by the Centers for Medicare & Medicaid Services (CMS), DSH operates under statutory formulas that determine funding limits, eligibility standards, and reporting obligations for each participating state.
1. DSH Eligibility and Qualification Criteria
- To qualify for DSH payments, hospitals must demonstrate a disproportionate share of Medicaid and low-income patients as defined under Section 1923(b) of the Social Security Act.
- Key federal criteria include:
- The hospital’s Medicaid inpatient utilization rate (MIUR) or low-income utilization rate (LIUR) must exceed statutory minimums.
- States may define additional qualifying thresholds in their State Plan Amendments (SPAs), subject to CMS approval.
- Both public and private hospitals can qualify if they meet the low-income utilization standards and provide uncompensated or undercompensated care to Medicaid beneficiaries.
- Hospitals that meet these requirements are designated as DSH-eligible institutions and may receive payments from the state’s DSH allotment.
2. DSH Funding Structure
- Each state receives an annual federal DSH allotment, which caps the total federal financial participation (FFP) available.
- States must contribute their non-federal share using Intergovernmental Transfers (IGTs) or Certified Public Expenditures (CPEs).
- DSH payments are made outside of standard Medicaid base rates and are reported separately to CMS for audit and tracking.
- DSH funds cannot duplicate payments made through UPL (Upper Payment Limit) or managed care arrangements.
3. DSH Payment Calculation and Distribution
- States develop payment methodologies via SPAs, defining how DSH funds are distributed among qualifying hospitals.
- Distribution may be based on uncompensated-care costs, Medicaid utilization, or hospital size and ownership type.
- CMS reviews each SPA to ensure payment equity and compliance with federal DSH allotment limits.
- Hospitals may receive multiple DSH adjustments per year, depending on state payment cycles and budget timing.
4. Federal and State DSH Allotments
- DSH funding is determined by statutory allotment formulas under Section 1923(f).
- Key aspects include:
- The total national DSH cap is established annually by CMS and divided among states.
- Each state’s allotment is based on historical spending patterns and adjusted for inflation and population factors.
- States that did not operate DSH programs in the baseline year receive minimum allotments, while high-utilization states (e.g., CA, NY, TX) receive larger allocations.
- Federal DSH caps are separate from state budget caps but both must align to maintain FFP eligibility.
5. Reporting, Auditing, and Compliance Requirements
- States must submit annual DSH reports and independent audits demonstrating that payments comply with federal limits.
- Reports must identify each DSH hospital, the payment amount, and the methodology used to calculate eligibility and costs.
- Audits verify that total DSH payments do not exceed hospital-specific limits (the hospital’s uncompensated care cost minus payments received from Medicaid and uninsured patients).
6. DSH vs. UPL: Complementary but Distinct Mechanisms
- While both programs serve to enhance Medicaid provider reimbursement, DSH and UPL (Upper Payment Limit) differ in scope and purpose:
- DSH targets hospitals with disproportionate low-income or uninsured patient loads.
- UPL applies a payment ceiling to all Medicaid reimbursement to ensure aggregate payments remain below Medicare-equivalent levels.
- States often coordinate both programs through their SPAs, aligning DSH funding with UPL compliance to maximize provider support without exceeding federal caps.
7. Policy Goals and Equity Objectives
- DSH programs aim to maintain access to essential inpatient and emergency care for vulnerable populations. By offsetting the uncompensated care burden, they strengthen safety-net hospitals and promote equity in healthcare delivery, particularly in rural and urban underserved areas.
- Failure to comply can result in federal disallowances or recoupment of funds.
How Disproportionate Share Hospital (DSH) Payments Work in Practice
The Disproportionate Share Hospital (DSH) program functions as a targeted supplemental payment mechanism that allows states to support hospitals serving a high proportion of Medicaid and uninsured patients.
While federally regulated, the program’s execution, eligibility management, and reporting are primarily handled by state Medicaid agencies under CMS oversight.
Step 1: Establishing State Plan Parameters
- Each state defines DSH program criteria and payment methodologies within its Medicaid State Plan.
- Changes to eligibility, formulas, or payment timing require submission of a State Plan Amendment (SPA) to CMS.
- CMS reviews the SPA for compliance with Section 1923 of the Social Security Act, ensuring alignment with national DSH funding caps and hospital-specific limits.
- Once approved, the state may begin distributing DSH payments according to its authorized plan.
Step 2: Identifying Eligible Hospitals
- States determine DSH eligibility based on the Medicaid Inpatient Utilization Rate (MIUR) and/or the Low-Income Utilization Rate (LIUR).
- Hospitals submit annual cost reports and utilization data documenting Medicaid and low-income patient volumes.
- States may include additional qualifying conditions, such as ownership status (public/private) or trauma center designation, within CMS-approved parameters.
- Eligible hospitals are designated as DSH providers for the fiscal year.
Step 3: Calculating Payment Amounts
- States use approved payment formulas—often based on uncompensated-care costs or Medicaid utilization—to determine each hospital’s DSH payment.
- Payments are subject to two key limits:
- The statewide DSH allotment (federal cap on total funding).
- The hospital-specific limit, which restricts payments to each facility’s uncompensated-care cost.
- DSH payments are generally issued on a quarterly or biannual basis, depending on the state’s budget structure.
Step 4: Distributing Funds
- States transfer the non-federal share through Intergovernmental Transfers (IGTs) or Certified Public Expenditures (CPEs) to draw down the federal match.
- Payments are processed through the state’s Medicaid Management Information System (MMIS) and recorded separately from standard claims payments.
- Funds are typically disbursed to hospitals as lump-sum supplemental payments, not tied to individual claims.
- CMS monitors the timing and reconciliation of payments to ensure compliance with both federal and state caps.
Step 5: Reporting and Annual Auditing
- States must submit DSH reports and independent audits each year to demonstrate compliance with statutory limits.
- Audits must verify that DSH payments do not exceed each hospital’s uncompensated-care cost and that no duplication occurs with other funding streams such as UPL or Medicaid managed care directed payments.
- CMS and the Office of Inspector General (OIG) review audit results and may issue disallowances or require corrective action if noncompliance is identified.
- Maintaining detailed, audit-ready documentation is essential for federal financial participation (FFP) retention.
Step 6: Program Adjustments and Federal Oversight
- CMS evaluates DSH programs through regional office reviews, state reports, and OIG audits.
- If findings reveal overpayments or inconsistent methodologies, CMS can:
- Require repayment of the federal share, or
- Mandate plan revisions via updated SPAs.
- States often refine DSH formulas annually to maintain alignment with hospital utilization trends and budgetary shifts.
- CMS also provides technical assistance and policy updates through State Medicaid Director (SMD) letters and Informational Bulletins.
Step 7: Integration with Other Medicaid Funding Mechanisms
- DSH operates in tandem with other Medicaid financing programs:
- UPL (Upper Payment Limit) – Ensures aggregate state Medicaid payments do not exceed Medicare-equivalent ceilings.
- IGTs (Intergovernmental Transfers) and CPEs (Certified Public Expenditures) – Finance the state share of DSH payments.
- SPAs (State Plan Amendments) – Serve as the policy vehicle for structural or formulaic updates.
- Coordination among these mechanisms helps states maintain budget neutrality while maximizing support for safety-net providers.
DSH in Medicaid Billing, Reimbursement, and Fiscal Limitations
Disproportionate Share Hospital (DSH) Payments are a critical part of Medicaid’s hospital reimbursement framework, providing financial stability to hospitals serving a high proportion of low-income patients. However, DSH is also among the most audited and compliance-sensitive funding mechanisms in the program, requiring strict adherence to both federal caps and state-level payment methodologies.
How DSH Affects Medicaid Reimbursement
- DSH payments operate as supplemental adjustments, made in addition to base Medicaid reimbursement.
- Each state’s annual DSH allotment establishes the ceiling for total federal participation (FFP) in that fiscal year.
- Payments are distributed based on state-defined formulas approved through State Plan Amendments (SPAs) and must comply with Section 1923(f) hospital-specific limits.
- Federal matching is available only for the portion of DSH payments that can be demonstrated as covering uncompensated-care costs.
- Accurate DSH implementation ensures that safety-net hospitals remain solvent and able to sustain Medicaid service delivery.
Funding Flow and Federal Matching
- DSH funding follows a shared financing model, combining:
- Federal funds (up to the state’s DSH allotment).
- Non-federal share (funded through Intergovernmental Transfers (IGTs) or Certified Public Expenditures (CPEs)).
- Once the state’s share is certified and transferred, CMS releases the federal matching funds (FMAP).
- States distribute DSH payments—typically quarterly—to eligible hospitals via lump-sum disbursements.
- CMS monitors FFP claims to ensure alignment between reported expenditures and audit-verified data.
Administrative and Data Limitations
- DSH administration is data-heavy, relying on accurate cost reports and uncompensated-care data.
- Errors in cost modeling or outdated financial inputs can result in payment overages or disallowances.
- States often depend on third-party consultants or actuaries to perform the complex calculations needed for compliance.
- Inconsistent provider reporting or delayed audit cycles can distort future allotment accuracy.
- CMS requires states to maintain audit-ready documentation for at least three years after the DSH payment year.
Audit Exposure and Compliance Risks
- The Office of Inspector General (OIG) and CMS auditors routinely review DSH programs to verify compliance with federal allotments and hospital-specific limits.
- Common audit findings include:
- Misapplied cost data or incorrect calculation of uncompensated-care costs.
- Payments exceeding the hospital-specific DSH limit.
- Overlapping funding with UPL, managed care directed payments, or other supplemental programs.
- When noncompliance is found, CMS may recoup the federal share or impose future payment restrictions.
- Proactive monitoring, accurate data integration, and transparent documentation are essential to minimize audit risk.
Fiscal Constraints and Reform Considerations
- Federal law currently imposes annual reductions in DSH allotments, intended to reflect declining uncompensated-care needs following coverage expansion under the Affordable Care Act (ACA).
- Implementation of these DSH cuts has been repeatedly delayed by Congress, but remains a key budgetary risk for states.
- As uncompensated-care patterns evolve, CMS continues to explore reforms linking DSH payments to quality metrics, equity goals, and transparency standards.
- Many states advocate for modernized DSH methodologies that integrate value-based payment principles without jeopardizing core safety-net funding.
How DSH Payments Influence Quality, Access, and Equity in Medicaid
The Disproportionate Share Hospital (DSH) program plays a central role in sustaining healthcare access for low-income and uninsured populations. Although primarily a financial stabilization tool, DSH also functions as a key instrument for health equity, ensuring that vulnerable communities retain access to essential hospital and emergency services despite lower reimbursement rates.
Supporting Access Through Financial Stability
- DSH payments help maintain the viability of safety-net hospitals, public teaching institutions, and urban and rural medical centers with large Medicaid populations.
- These facilities provide disproportionate levels of uncompensated care, often operating with negative margins without DSH support.
- By offsetting these losses, DSH ensures that hospitals can continue offering emergency, trauma, and obstetric services to Medicaid and uninsured patients.
- Without DSH funding, many hospitals in underserved areas would face service cutbacks or closures, threatening community-level access to care.
Equity in Hospital Reimbursement and Resource Allocation
- DSH allocations are designed to reduce geographic and socioeconomic disparities in Medicaid hospital funding.
- By targeting institutions with the highest low-income and uninsured utilization rates, DSH promotes payment equity across hospitals that serve different populations.
- However, variability in state-level methodologies can create regional inconsistencies—where some hospitals receive disproportionate funding advantages.
- CMS continues to encourage states to adopt transparent, data-driven formulas that prioritize hospitals serving the greatest community need.
Transparency and Accountability in DSH Administration
- DSH programs have historically faced scrutiny for opaque distribution processes and limited public visibility into payment methodologies.
- CMS now requires annual independent audits and public reporting of DSH payments, ensuring accountability in how funds are allocated.
- Transparency reforms enable policymakers, community stakeholders, and hospital systems to better assess whether DSH funding aligns with actual uncompensated-care burdens.
- Enhanced reporting also supports cross-program coordination between DSH, UPL, and Medicaid managed care financing.
Impact on Quality of Care
- Stable DSH funding allows hospitals to invest in clinical staffing, infrastructure, and quality improvement initiatives that benefit all patients—not just Medicaid enrollees.
- Sustained financial support through DSH can help reduce readmission rates, overcrowding, and care delays often associated with underfunded facilities.
- Hospitals that receive predictable DSH payments are better positioned to maintain quality compliance, accreditation, and staff retention, which directly improve patient outcomes.
- CMS’s emerging value-based DSH initiatives seek to link portions of supplemental funding to performance on quality and equity measures.
DSH and the Broader Equity Framework
- DSH complements CMS’s broader health equity and access goals by addressing structural underfunding in safety-net care delivery.
- The program helps counterbalance systemic inequities that result from geography, income, and coverage gaps.
- By maintaining the financial stability of institutions that disproportionately serve communities of color and rural regions, DSH supports equitable access at both the state and national levels.
- As Medicaid transitions toward value-based and quality-linked reimbursement, DSH will remain a vital instrument for ensuring that equity and fiscal responsibility coexist within the public healthcare safety net.
